Detection of Hearing Impairment in Patients with Subjective Complaints of Hearing Loss using the Whispered Voice Test and Standard Pure Tone Audiometry: A Prospective Non-Randomized Trial
Giselle L. Gotamco, Norberto V. Martinez,
Sep 2017 DOI 10.35460/2546-1621.2017-0008
INTRODUCTION
Disabling hearing loss is defined as hearing loss greater than 40 decibels and 30 decibels in the better hearing ear in adults and in children, respectively, and affects 360 million people worldwide.(1) Regardless of the cause, hearing impairment substantially disturbs communication, leading to academic,social and economic disadvantage.(1,2) In Philippines, the hearing loss is estimated to affect 5.64 to 36% of the total population. Consequently, 56.4% and 67.7% of those with hearing disability were not able to complete high school education and had no income-generating job respectively.(3)
Knowing the sequelae of hearing impairment emphasizes the need for methods to detect it through a simple yet reliable test that could be performed easily by ENT specialists and general practitioners alike. Hearing impairment is a modifiable problem once it is detected. Early recognition of the problem leads to earlier intervention and rehabilitation, preventing it disabling effects.
The standard tools for the detection of hearing impairment have limitations in our setting wherein access to specialists and audiometric evaluation is not always possible. Formal audiometric testing requires time, training and technology that are not readily available. Screening through the whispered voice test (WVT) is an alternative that can be used to identify individuals that warrant further evaluation by ENT specialists. It is relatively simple and has been tested in both adults and children however, it lacks standardization, compromising its application in the primary care setting.
This study aims to determine the accuracy of the whispered voice test compared to standard pure tone audiometry in detecting hearing impairment in patients with subjective complaints of hearing loss and to determine the association of pure tone audiometry and whispered voice test results to the age of the subjects as well as to each other.
METHODOLOGY
This is a prospective, non-randomized trial done in a tertiary private hospital. A total of 55 consecutive patients aged 13- to -85 year old who underwent hearing evaluation via pure tone audiometry were included in the study.
Two examiners performed pure tone audiometry and whispered voice tests independently and blindly. The tests were performed one after the other in no particular order.
Pure tone audiometry averages for each ear were interpreted and recorded based on the institution’s reference, the World Health Organization Hearing Loss Classification as follows: normal (0-25dB), mild (26-40dB), moderate (41-60 dB), severe (61-80 dB), and profound (81dB and above).
The whispered voice test was performed in a room with no soundproofing to mimic the natural environment and ambient noise in consultation clinics. Subjects were seated and instructed to occlude the test ear by pushing the tragus over the external auditory canal. The examiner stands one meter behind the subject, whispers numbers after a quiet exhale, and asks the subject to repeat them. Garnering more than 50% correct responses corresponds to passing the whispered voice test. Failure to give more than 50% correct responses corresponds to failing the whispered voice test. In subjects who failed the whispered voice test, gradation to conversational (C) voice or loud (L) voice was done as necessary. The voice level wherein the subject gives more than 50% correct responses were noted. Failure to give more than 50% correct responses or no response on loud voice corresponded to no reaction (NR). The same procedure is done on the contralateral ear.
The researcher summarized the subjects’ characteristics and findings using percentages for dichotomous variables and means with standard deviations for continuous variables. Frequencies and means (± standard deviation) were used to describe the demographic data. Specificity, sensitivity, positive and negative predictive values, positive and negative likelihood ratios, and accuracy of the whispered voice test against standard pure tone audiometry were determined. The associations of the whispered voice test and pure tone audiometry to each other and to age were also established.
Statistical analyses were performed using SPSS (version 21; SPSS Inc., Chicago, IL USA) software considering 95% confidence interval in demographic data analyses. Cross tabulations were displayed and examined. To assess the prevalence of patients with hearing loss and the significant difference between the expected and observed result on demographic profile, the whispered voice test, and standard pure tone audiometry results, the researcher performed cross tabulation and Chi square test. Additional statistical tests to estimate the sensitivity, specificity, positive and negative predictive values, positive and negative likelihood ratios, and accuracy of the whispered voice test in detecting hearing loss were also done.
RESULTS
The data on age and gender were tabulated and presented in frequency and percentage as shown in Table 1. 55 patients were included with a total of 110 ears studied. It was revealed that 40% (n=22) are males while the remaining 60% (n=33) are females. With the above numbers, the gender ratio is approximately 2 male patients for every 3 female patients (2:3). The patients’ ages ranged from 13 to 85 years old with an average of 44.99. Cross tabulation of respondents’ age and whispered voice test result was done. Early 30’s respondents acquired the highest frequency of normal hearing and late 60’s respondents obtained a lower frequency of normal hearing when categorized using the whispered voice test. The Pearson’s chi-square was 68.24 with degrees of freedom of 27. Using 0.05 level of significance, the p-value was 0.000. Generally, there is significant association between age and whispered voice test. Similarly, cross tabulation of age and pure tone audiometry result was done. The ages of the respondents with normal hearing threshold were distributed in the age interval of 18-58 years. The chi-square value of age and pure tone audiometry was 70.52. The p-value between two variables was less than 0.05. Generally, the statistical analysis shows that there is significant association between age and pure tone audiometry.
The frequency distribution of the whispered voice test and pure tone audiometry results are shown in Table 2. The results indicated that 64 (58.2%) ears passed the whispered voice test and 46 (41.8%) ears were identified as hearing impaired by the whispered voice test. It was observed that 65 (59.1%) had normal hearing threshold and 45 (40.9%) suffered some degree of hearing loss as documented by pure tone audiometry.
Cross tabulation of whispered voice test and pure tone audiometry is shown in (Table 3). Sixty ears with normal hearing threshold on pure tone audiometry were correctly identified by the whispered voice test. Five ears assessed by pure tone audiometry with normal hearing did not correctly respond to the whispered voice test. Four ears with hearing loss as assessed by pure tone audiometry passed the whispered voice test. The chi-square value of whispered voice test and pure tone audiometry was 151.59 with degrees of freedom equal to 27. The p-value of 0.000 was less than 0.05. Generally, the statistical analysis shows that there is significant association between whispered voice test and pure tone audiometry.
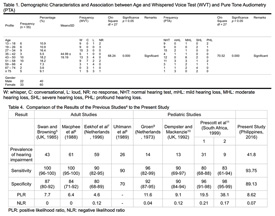
The sensitivity and specificity of the whispered voice test were 93.75% and 89.13%, respectively. Positive predictive value was 92.31% while the negative predictive value was 91.11%. The positive and negative likelihood ratios were 8.62 and 0.07, respectively with a computed accuracy of 91.82%.These results are tabulated against the results of previous studies4 (Table 4).
DISCUSSION
Accuracy of the Whispered Voice Test
The sensitivity and specificity of the whispered voice test in this study was comparable to previous studies. In a systematic review by Pirozzo et al.,(4) the whispered voice test yielded a sensitivity of 82-100% and a specificity of 70-87% in adults. The prevalence of hearing impairment in this population was 26-61%. In the same study, it yielded a sensitivity of 61-99% and a specificity of 84-99% in the pediatric population. The prevalence of hearing impairment in this population was 9-31%. The likelihood ratios and the prevalence of hearing impairment in this study are likewise comparable to the studies reviewed by Pirozzo. In the study of Swan and Browning, (5) a total of 202 ears among 17- to 89-year-old were studied. Occlusion of the non-test ear was done for masking and the tester stood behind the patient to avoid lipreading. Eekhof, (7) on the other hand, included 124 ears belonging to adults 55 years old and above only. The sensitivity and specificity of the whispered voice test was compared to Pat 225, Audioscope-3, and Micromate-304. Among these, the whispered voice test was the least expensive and relatively, had high sensitivity and specificity compared to the other tests. Both the Audioscope-3 and Micromate-304 had a sensitivity of 100% however, sensitivity were low at 42% and 39%, respectively. The tests were also done in a generic consultation room with no sound-proofing. Test of interobserver reliability showed variable outcomes among examiners owing to the non-standardized volume of the whisper used. Groen (9) included a total of 197 5-year-old children in his study. In his method, the test was done starting at a 3-meter distance, with occlusion of the non-test ear and using spondee words. Testers for the whispered voice test and audiogram halfway into the test to minimize biases. Dempster and Mackenzie’s (10) study also included only the pediatric age group composed of 141, 5- to 12-year old children using used numbers and/or letters. Masking was achieved by tragal rubbing of the non-test ear. Since there was no significant difference in the results of the right and left ear, only data from the right ear were presented. Two independent observers did the test in a generic out-patient setting but did not included a test using non-specialists. Prescott (11) initially confirmed assumptions on the human voice prior to implementing his study (whisper: 30-45dB, conversational voice: 45-60 dB, and loud voice: 60-80 dB). He then proceeded with a hospital based study composed of 177, 3- to 12-year-old children. This was followed by a school-based study composed of 201 3- to 7-year-olds. Spondee words were used in this study.
The values obtained for sensitivity (93.75%) and specificity (89.13%) of the whispered voice test in this study make it a reliable screening test for hearing loss. The likelihood ratios are favorable to the whispered voice test as well. The positive likelihood ratio of 8.62 means that failing the whispered voice test corresponds to a moderate increase in the likelihood of having hearing loss while the negative likelihood ratio of 0.07 means that passing the whispered voice test corresponds to a large and conclusive decrease in the likelihood of having hearing loss.
The whispered voice test missed the diagnosis of hearing loss in four (3.6%) samples. The four false negative responses on whispered voice test had pure tone audiometry averages of 26.67, 28.33, 26.6, and 45. Prescott et al., observed a similar discrepancy, albeit at a higher incidence of 25% but also along the average of mild hearing loss. (11) The outlier positive response to the whispered voice test despite the finding of moderate hearing loss on pure tone audiometry may be explained by an inadequately covered external auditory canal that allowed cross over as this subject had normal hearing threshold on the contralateral ear. The five ears that were incorrectly identified as having hearing loss had pure tone averages well within normal threshold at 13.33 in two samples, 20, 23.33, and 15. The false positive responses on whispered voice test may be due to ambient noise preventing the subject from interpreting the whispered voice signals.
The positive predictive value indicates the percentage of samples that failed the whispered voice test that actually have hearing loss. On the other hand, the negative predictive value indicates the percentage of samples that passed the whispered voice test that have normal hearing threshold. The positive and negative predictive values of the whispered voice test are 92.31% and 91.11%, respectively. This implies that less than 10% of those who failed the whispered voice test will have normal hearing and that passing the whispered voice test reliably indicates normal hearing.
Association of Whispered Voice Test with Age
This study showed a sample predominantly composed of females (60%) with a ratio of 3:2 to males (40%) with a mean age of 44.99 ± 19.19 years. The populations wherein age-related changes in hearing can be observed (12) and that would highly benefit from screening are well represented. This study was composed of men and women aged 48-85 years who underwent a screening test to determined the sensitivity of a portable audiometer and results show similar detection rates to previous studies. Approximately 10% (n=6) of the subjects belonged to the pediatric age group (d 18 years old) wherein the prevalence of hearing impairment is generally lower at 1.65%,(13) after total ascertainment of children with hearing impairment and a capture-recapture analysis in the United Kingdom.
Based on the results, majority of the ears with a normal response to the whispered voice test were equally distributed among the different age intervals. Moreover, the samples falling in the range of 59 years old and above represent the smallest portion of the ears with normal hearing on whispered voice test. The chi-square value between age and whispered voice test was 68.24 using 5% level of significance. Age was significantly associated with the whispered voice test of the patients (p = 0.000). Likewise, majority of the ears with normal hearing threshold on pure tone audiometry belonged to the d 18 to 58 year olds. The chi-square value between age and pure tone audiometry was 70.52 using 5% level of significance. Age was significantly associated with the pure tone audiometry of the patients (p = 0.000). This data is further verified by Abutan BB, Sindhusake D and Cruickshanks KJ, who concluded that 40% of people aged more than 60 and by 90% of people aged more than 80 are affected by hearing impairment.(4)
64 ears (58.2%) responded normally in the whispered voice test while 65 ears (59.1%) were documented to have normal hearing threshold on pure tone audiometry. The tabulated results of the whispered voice test and pure tone audiometry were very similar with a percentage difference of 0.9%. Comparatively, the percentage of ears with no response in whispered voice test and profound hearing loss on pure tone audiometry were also very similar with a percentage difference of 1.8%. The Pearson chi-square value of whispered voice test and pure tone audiometry was 151.59 with p = 0.000. Significant association was found between the two procedures.
CONCLUSION
The whispered voice test is an accurate (91.82%) screening tool in the detection of hearing loss. The whispered voice test and pure tone audiometry results are associated with age and with each other. ENT specialists and general practitioners in the rural and urban settings can use it as a preliminary test prior to requesting routine pure tone audiometry in patients with subjective complaints of hearing loss. The test can be done with no need for formal training, in a short amount of time, and in typical clinic conditions. However, it does not have the ability to differentiate among the different types of hearing loss and distinguish between high- and low-frequency hearing losses.
We recommend the inclusion of more pediatric patients in the study as well as an overall increase in the number of subjects. The success of the test is dependent on the subject’s ability to follow instructions hence it is important to always ensure that the external auditory canal is properly and adequately occluded in order to prevent false negative results. The addition of tragal rubbing can further prevent the occurrence of false negative results. Furthermore, using spondee words or a combination of letters instead of numbers can provide a different perspective in the implementation of the test in that it can potentially classify subjects into those with high- and low-frequency hearing loss.
- World Health Organization. Global Estimates on Prevalence of Hearing Loss. Mortality and Burden of Diseases and Prevention of Blindness and Deafness. 2012.
- Stevens G, Flaxman S, Brunskill E, Mascarenhas M, Mathers C, Finucane M, et al. Global and regional hearing impairment prevalence: an analysis of 42 studies in 29 countries. European Journal of Public Health. 2011 December 24;23:146–152.
- Yap J, Reyes C, Albert JR, Tabuga A. Philippine Institute for Development Studies. Preliminary results of the survey on PWDs conducted in selected metro manila cities. PIDS Discussion Paper Series. 2009 August;25
- Pirozzo S, Papinczak T, Glasziou P. Whispered voice test for screening for hearing impairment in adults and children: systematic review. BMJ 25 October 2003;327.
- Swan IR, Browning GG. The whispered voice as a screening test for hearing impairment. J R Coll Gen Pract 1985;35:197.
- Macphee GJ, Crowther JA, McAlpine CH. A simple screening test for hearing impairment in elderly patients. Age Ageing 1988;17:347-51.
- Eekhof JA, de Bock GH, de Laat JA, Dap R, Schaapveld K, Springer MP. The whispered voice: the best test for screening for hearing impairment in general practice? Br J Gen Pract 1996;46:473-4.
- Uhlmann RF, Rees TS, Psaty BM, Duckert LG. Validity and reliability of auditory screening tests in demented and non-demented older adults. J Gen Intern Med 1989;4:90-6.
- Groen JJ. Pure tone audiometry and whispered voice test. Conformities and differences in tests results. ORL J Otorhinolaryngol Relat Spec 1973;35:65-70.
- Dempster JH, Mackenzie K. Clinical role of free-field voice tests in children. Clin Otolaryngol 1992;17:54-6.
- Prescott CA, Omoding SS, Fermor J, Ogilvy D. An evaluation of the “voice test” as a method for assessing hearing in children with particular reference to the situation in developing countries. Int J Pediatr Otorhinolaryngol 1999;51:165-70.
- Cardoso, CL, et al. Sensitivity and specificity of portable hearing screening in middle-aged and older adults. Int. Arch. Otorhinolaryngol. 2014;18(1):21-26.
- Fortnum HM, Summerfield AQ, Marshall DH, Davis AC, Bamford JM. Prevalence of permanent childhood hearing impairment in the United Kingdom and implications for universal neonatal hearing screening: questionnaire based ascertainment study. BMJ 2001;323:536-40.
TABLES
Table 1. Demographic Characteristics and Association between Age and Whispered Voice Test (WVT) and Pure Tone Audiometry
|
Profile |
Frequency (n=55) |
Percen tage (%) |
Mean ± SD |
Frequency (WVT) |
Chi-Square df = 27 |
Significance p = 0.05 |
Remarks |
Frequency (PTA) |
Chi-Square df = 27 |
Significance p = 0.05 |
Remarks |
|||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
W |
C |
L |
NR |
NHL |
mHL |
MHL |
SHL |
PHL |
||||||||||
|
13-18 19-26 27-34 35-42 43-50 51-58 59-66 67-74 >=75 |
6 6 9 3 10 10 4 2 5 |
10.9 10.9 16.4 5.5 18.2 18.2 7.3 3.6 9.1 |
44.99± 19.19 |
9 9 15 5 13 9 3 0 1 |
0 0 3 1 3 7 1 3 5 |
1 0 0 0 4 2 4 1 3 |
2 3 0 0 0 2 0 0 1 |
68.24
|
0.000
|
Significant
|
9 9 15 4 12 11 3 1 1 |
0 0 2 1 0 3 1 1 3 |
1 0 1 1 6 3 2 2 0 |
0 2 0 0 2 1 1 4 2 |
2 1 0 0 0 2 1 0 1 |
70.52
|
0.000
|
Significant
|
W: whisper, C: conversational, L:loud, NR: no response, NHT: normal hearing test, mHL: mild hearing loss, MHL: moderate hearing loss, SHL: severe hearing loss, PHL: profound hearing loss
Table 2. Frequency Distribution of Whispered Voice Test (WVT) and Pure Tone Audiometry (PTA)
|
Profile |
Frequency (n = 110) |
Percentage (%) |
|---|---|---|
|
WVT Whisper (W) Conversational (C) Loud (L) No Response (NR) |
64 23 15 8 |
58.2 21.9 13.6 7.3 |
|
PTA Normal Hearing Threshold (NHT) Mild Hearing Loss (mHL) Moderate Hearing Loss (MHL) Severe Hearing Loss (SHL) Profound Hearing Loss (PHL) |
65 12 15 12 6 |
59.1 10.9 13.6 10.9 5.5 |
Table 3. Association between Whispered Voice Test (WVT) and Pure Tone Audiometry (PTA)
|
Description |
Frequency (WVT) |
Chi-Square df = 27 |
Significance p = 0.05 |
Remarks |
|||
|---|---|---|---|---|---|---|---|
|
W |
C |
L |
NR |
||||
|
PTA NHT mHL MHL SHL PHL |
60 3 1 0 0 |
5 7 9 2 0 |
0 1 6 7 1 |
0 0 0 3 5 |
151.59 |
0.000 |
Significant |
NHT: normal hearing threshold, mHL: mild hearing loss, MHL: moderate hearing loss, SHL: severe hearing loss, PHL: profound hearing loss, W: whisper, C: conversational, L: loud, NR: no response.
Table 4. Comparison of the Result of the Previous Studies4 to the Present Study
|
Result |
Adult Studies |
Pediatric Studies |
|
||||||
|---|---|---|---|---|---|---|---|---|---|
|
|
Swan and Browning (UK, 1985) |
Macphee el al6 (1988) |
Eekhof et al7 (Netherlandss, 1996) |
Uhlmann et al8 (1989) |
Groen9 (Netherlands, 1973 |
Dempster and Mackenzie10 (UK, 1992) |
Prescott et al11 (South Africa, 1999) |
Present Study (Philippines, 2016) |
|
1 |
2 |
||||||||
Prevalence of hearing impairment |
43 |
61 |
59 |
26 |
14 |
13 |
31 |
9 |
41.8 |
|
Sensitivity |
100(96-100) |
100(95-100) |
90(82-95) |
90 |
96(82-99) |
90(69-97) |
80(68-88) |
83(61-94) |
93.75 |
|
Specificity |
87(80-92) |
84(71-92) |
80(68-89) |
70 |
92(87-95) |
90(84-94) |
96(91-98) |
98(95-99) |
89.13 |
|
PLR |
7.7 |
6.4 |
4.6 |
- |
11.6 |
9.1 |
19.5 |
38.1 |
8.62 |
|
NLR |
0 |
0 |
0.12 |
- |
0.04 |
0.12 |
0.12 |
0.17 |
0.07 |
DISCLOSURE AND CONFLICT OF INTEREST
The authors have no financial or other (including personal) relationships, intellectual passion, political or religious belief, and institutional affiliations that might lead to a conflict of interest.
![]() CC BY:
Open Access Creative Commons Attribution 4.0 International
License, which permits use, sharing, adaptation, distribution and
reproduction in any medium or format, as long as you give
appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if
changes were made. The images or other third party material in
this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material.
If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this
license, visit http://creativecommons.org/licenses/by/4.0/
CC BY:
Open Access Creative Commons Attribution 4.0 International
License, which permits use, sharing, adaptation, distribution and
reproduction in any medium or format, as long as you give
appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if
changes were made. The images or other third party material in
this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material.
If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this
license, visit http://creativecommons.org/licenses/by/4.0/