Risk Factors and Clinical Outcomes of Hospitalized Covid-19 Patients with Diabetes Mellitus in a Tertiary Hospital
Jiselle Aimee Y. Bedia, Maria Honolina S. Gomez, Jean Uy-Ho, Erick S. Mendoza, Lizette Kristine F. Lopez
Apr 2025 DOI 10.35460/2546-1621.2023-0020

Introduction
Diabetes mellitus type 2 is a major lifestyle disease that has affected 463 million people worldwide. The last three decades showed an epidemic rise in the number of people with type 2 diabetes mellitus (T2DM), especially in South-East Asia. [1,2]
In corollary to this, the coronavirus-19 (COVID-19) pandemic has shocked the global community with 35 million confirmed cases as of October 2020.[ 3,4] The clinical spectrum of COVID-19 is heterogeneous, ranging from mild symptoms to severe or critical disease and sometimes death.[3] A recent meta-analysis showed that the prevalence of diabetes in COVID-19 infection ranged from 10% to 20%.[3] Since the virus’ first appearance in December 2019 in China, medical experts have focused their attention to individuals with diabetes because of its worse prognosis and high healthcare cost.[5] Moreover, diabetes is known to confer an increased risk for infections, particularly respiratory infections.[5] Because of its high prevalence, diabetes has become a frequent comorbidity in patients affected with COVID-19. [6]
The relationship between T2DM and COVID-19 is brought about by hyperglycemia and insulin resistance, which promotes oxidative stress and the release of pro-inflammatory mediators. As a result, this inflammatory process leads to a higher propensity for infections resulting in worse complications. [7] In a recent meta-analysis, the presence of diabetes was associated with severe COVID-19 infection and mortality with a pooled odds ratio of 2.75 and 1.9, respectively. This was attributed to multiple immune dysregulation such as phagocytic cell dysfunction, inhibition of neutrophil chemotaxis, impaired T-cell mediated immune response, altered cytokine production and ineffective microbial clearance leading to increased levels of inflammatory mediators. The study also found that the presence of diabetes in patients with COVID-19 increases the risk of disease severity and mortality two-fold as compared to patients without diabetes. [8] Patients with newly diagnosed diabetes have the highest risk for developing complications and all-cause mortality compared to those patients with known diabetes. This is due to stress-induced hyperglycemia leading to a significant increase in the risk of severe disease and poorer prognosis. [9] The clinical characteristics of COVID-19 patients with diabetes mellitus show that most of these patients were elderly without any exposure history, but had at least one comorbid condition, namely, hypertension, cardiovascular disease, and a history of cerebrovascular disease.[10]
A wide number of studies have been conducted to describe the clinical characteristics of COVID-19 patients with T2DM in different geographic locations and ethnicities.[11-19] In the Philippine setting, the clinical profile of Filipino patients who get infected with COVID-19 are elderly males without recent travel history but with concurrent hypertension, diabetes mellitus and respiratory disease.[11] Similarly, a study done in the United Kingdom found that COVID-19 patients with T2DM tend to be older with lower probability of survival and longer hospitalization stay.[17] In developing countries with limited healthcare allocation such as the Philippines, a significant subset of the Filipino population still gets infected because not all Filipinos follow the mandate of self-isolation and proper respiratory etiquette protocols. Among those vulnerable patients are individuals with diabetes mellitus.
Due to the observed relationship between T2DM and COVID-19 infection, this study aimed to determine the risk factors affecting clinical outcomes of hospitalized COVID-19 patients with diabetes mellitus admitted at the University of Santo Tomas (UST) Hospital. Specifically, it aims to determine the prevalence of diabetes mellitus among admitted patients with COVID-19, to identify and associate the risk factors influencing disease prognosis among COVID-19 patients with diabetes mellitus, to determine the association of risk factors, glycemic status and prior medication use as to the length of hospitalization and COVID-19 severity, to determine the association of risk factors, glycemic status and prior medication use and its effect on disease morbidity, mortality and recovery, and to identify the clinical profile of COVID-19 patients with diabetes mellitus and correlate their clinical outcome as to disease severity, length of hospitalization, intensive care unit (ICU) admission, morbidity, recovery and mortality.
Methodology
Study Design and Participants
This is a retrospective cohort study conducted in the UST Hospital. This study involved all patients with diabetes mellitus and COVID-19 infection admitted from March to October 2020.
Inclusion and Exclusion Criteria
This study included all Filipino patients aged 18 years old and above, with the Department of Health (DOH)-accredited laboratory-confirmed COVID-19 through real-time reverse transcription polymerase chain reaction (rRT-PCR) testing of nasopharyngeal or oropharyngeal specimens. The patients were admitted for at least 24 hours at the COVID ward. The subjects met the American Diabetes Association diagnostic criteria: fasting plasma glucose =/>7.0 mmol/L (=/>126 mg/dL) or 2-hour post-prandial glucose =/>11.1 mmol/L (>200 mg/dL), or HbA1c level =/>6.5%, for the diagnosis of diabetes mellitus. Excluded were mild COVID-19 positive patients who were not admitted and advised for home quarantine, patients whose medical records were not available at the records section or with incomplete data during data collection.
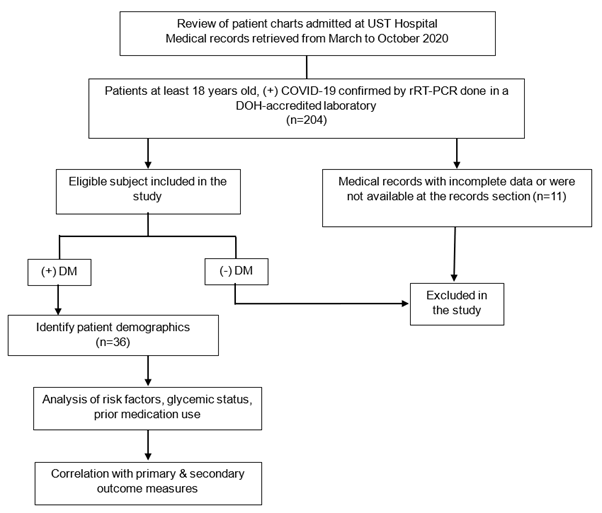
Figure 1. Flowchart of subject selection process
Data Collection
The UST Hospital - Research Ethics Committee (USTH-REC) approved this study and waived informed consent from the study participants because of the study’s retrospective design (approval # REC-2020-11-127-TF). Also, permission from the data privacy officer for the access of hospital patients’ records was secured prior to conduct of the study. A list of all COVID-19 patients admitted from March to October 2020 was taken from the Infection Prevention and Control Committee (IPCC) of the hospital. The charts of these admitted patients that included demographic, clinical, laboratory, treatment-related and outcome-related data were reviewed and extracted by the investigator using a standardized data collection form. Confidentiality and anonymity of each subject were ensured by giving each subject a unique subject code number. The primary investigator and statistician were the only ones who had access to the collected research data. Both paper and electronic copies of all research data will be disposed after three months from the time of data collection and statistical analysis.
Outcome Measures
Primary outcome measures:
-
Disease severity - COVID-19 severity classified as either mild, moderate, severe, or critical COVID-19 based on the World Health Organization (WHO) case definition.
-
Length of hospitalization - in number of days from day of admission up until day of discharge
Secondary outcome measures:
-
Admission in the intensive care unit (ICU)
-
Morbidity index - nonfatal myocardial infarction or nonfatal stroke during admission
-
Recovery - discharged from the hospital (as recommended by the attending physician) with evidence of clinical improvement.
-
Clinical improvement - absence of cough, fever, diarrhea, body malaise, sore throat; improvement of radiologic findings or total clearing of the pulmonary infiltrates; improvement in functionality and hemodynamic status
-
-
In-hospital mortality - mortality resulting from a clinically compatible illness in a probable or confirmed COVID-19 case (e.g., death from any cause namely, respiratory failure, myocardial infarction, and septic shock) during the hospital stay.
Data Analysis
Descriptive statistics such as mean and standard deviation were used to present continuous variables while frequencies and percentages were used for categorical data. Association of outcome to possible risk factors was done via univariate logistic regression. For variables where zero cells were present, Fisher’s exact test was utilized. Level of significance was at 5%. All statistical calculations were carried out using Medcalc Statistical Software version 19.6.
Definition of Terms
The following terms used or mentioned in this study were specifically defined for purposes of clarification.
As to the demographics, the following terms were used: (1) Body mass index (BMI) is defined as an actual weight (or last recalled weight or estimated weight) in kilograms (kg) divided by known or measured height in square meters (m2) and categorized according to the WHO International Obesity Task Force Asia-Pacific Classification [15], namely: underweight is a BMI of <18.5 kg/m2, normal weight is a BMI ranging from 18.5 to 22.9 kg/m2, overweight is a BMI ranging from 23 to 24.9 kg/m2 and obese is a BMI of ≥25 kg/m2; (2) Smoking history is categorized as current smoker (an adult who has smoked (either cigarette or tobacco) within the past 30 days from admission [20]), former smoker (an adult who has smoked (either cigarette or tobacco) in his or her lifetime, but has quit smoking for more than one month from admission [20]) and a non-smoker (an adult who has never smoked [20]); (3) Comorbid illnesses namely: hypertension, defined as an average blood pressure of at least 130/80 mmHg obtained on at least two separate occasions or as diagnosed by the physician or intake of anti-hypertensive medications [21]; atherosclerotic cardiovascular disease, defined as a history of coronary heart disease (CHD), cerebrovascular disease, or peripheral arterial disease presumed to be of atherosclerotic origin [22]; chronic kidney disease, defined as patients who are on maintenance dialysis, or has undergone renal transplantation, or with documented reduced kidney function (estimated glomerular filtration rate [eGFR] <90 mL/min2) for at least three months; non-alcoholic fatty liver disease (NAFLD), defined as fatty liver, non-alcoholic steatohepatitis, [23] or as diagnosed by the physician or based from subject’s history; neoplasm, defined as cancer of the breast, lung, prostate, colorectal, or hematologic, or any neoplasms diagnosed by the physician or based from subject’s history; respiratory disease, comprising either bronchial asthma, chronic obstructive pulmonary disease (COPD), bronchiectasis, tuberculosis or as reported by the subject. Moreover, the case definition of diabetes mellitus and glycemic status comprise either a known or physician-diagnosed T2DM or the use of glucose-lowering medications prior to admission. Diabetes is also defined based on the American Diabetes Association (ADA) criteria with a fasting plasma glucose (FBS) ≥126 mg/dL or Hba1c ≥6.5% or random blood sugar (RBS) >200 mg/dL with presence of classic symptoms of hyperglycemia (polydipsia, polyuria, polyphagia). On the other hand, newly diagnosed5diabetes mellitus is defined as the presence of at least two abnormal results of the following: FBS ≥126 mg/dL, HbA1c ≥6.5%, random blood sugar (RBS) ≥200 mg/dL, symptoms of hyperglycemia; without any history of diabetes or was never diagnosed with diabetes mellitus in the past. [16] Further, glycemic status is classified as to good glycemic control with an admission HbA1c level below or equal to 7%, fair glycemic control with an admission HbA1c level between 7% to 8.5%, and poorly controlled diabetes mellitus with an admission HbA1c level above 8.5%. Addendum, fasting blood glucose is categorically determined either as fasting plasma glucose (mg/dL), a standard method for measuring and reporting blood glucose concentrations after fasting (no food or drink) for at least 8 hours [25], or as fasting capillary blood glucose (mg/dL), a capillary sampling (through fingerstick pricking) measuring the glucose concentrations in the blood,[25] taken upon waking up in the morning.
As to the COVID-19 case definition, confirmed COVID-19 is defined as any adult at least 18 years of age who experiences any of the following symptoms: fever, cough, fatigue, anorexia, shortness of breath, myalgias, or non-specific symptoms (e.g., sore throat, nasal congestion, headache, diarrhea, nausea, vomiting, anosmia, ageusia); with laboratory confirmed positive rRT-PCR result through nasopharyngeal/oropharyngeal or lower respiratory tract aspirates. [18,26] It is further subdivided into its disease severity. Patients with mild disease are symptomatic patients meeting the case definition for confirmed COVID-19 without evidence of viral pneumonia or hypoxia.[18] Patients with moderate disease are any adult at least 18 years of age with clinical signs of pneumonia [fever, cough, dyspnea, fast breathing (respiratory rate ≥30 breaths per minute)] but no signs of severe pneumonia, including SpO2 ≥90% on room air; with chest imaging (ie, radiograph, chest CT scan) suggestive of the disease.[ 18] Patients with severe disease are any adult at least 18 years of age with clinical signs of pneumonia (fever, cough, dyspnea, fast breathing) plus one of the following: respiratory rate >30 breaths per minute, severe respiratory distress, or SpO2 <90% on room air; with chest imaging (ie, radiograph, chest CT scan) findings showing that the lesion progressed more than 50% within 24 to 48 hours.[18] Patients with critical disease are any adults with confirmed COVID-19 with acute respiratory distress syndrome (any adult at least 18 years of age with a disease onset within one week of a known clinical insult [i.e., pneumonia]) or new or worsening respiratory symptoms or as diagnosed by the attending physician; with chest imaging findings (i.e., radiograph, chest CT scan) of bilateral opacities, not fully explained by volume overload, lobar or lung collapse, or nodules; the origin of pulmonary infiltrates of respiratory failure is not fully explained by cardiac failure or fluid overload, as assessed by the attending physician [18]), sepsis (any adult at least 18 years of age with acute life-threatening organ dysfunction caused by a dysregulated host response to suspected or proven infection; signs of organ dysfunction include: altered mental status difficult or fast breathing, low oxygen saturation, reduced urine output, fast heart rate (>100 bpm, weak pulse, cold extremities, or low blood pressure (systolic blood pressure <90 mmHg, diastolic blood pressure <60 mmHg), skin mottling, laboratory evidence of coagulopathy, thrombocytopenia, acidosis, or high lactate [18]), or septic shock (any adult at least 18 years of age with persistent hypotension despite volume resuscitation, requiring vasopressor to maintain mean arterial pressure (MAP) ≥65 mmHg and serum lactate >2 mmol/L[18]). Moreover, chest imaging findings of COVID-19, as assessed by a radiologist are defined and determined through a chest radiograph or chest CT scan. Chest radiographic findings of COVID-19 may show characteristic signs such as bilateral “patchy” and/or “confluent, bandlike” ground glass opacity or consolidation in a peripheral and mid-to-lower lung zone distribution [26], or non-specific signs such as any pleuropulmonary abnormality other than the characteristic signs [26], or negative chest radiograph defined as no perceived pleuropulmonary abnormality.[ 26] In addition, chest CT scan may show typical COVID-19 findings such as peripheral, bilateral, ground-glass opacity with or without consolidation or visible intralobular lines (“crazy paving”); or multifocal ground-glass opacity of rounded morphology with or without consolidation or visible intralobular lines (“crazy paving”); or reverse halo sign or other findings of organizing pneumonia, [19] or indeterminate findings such as absence of typical features and presence of either: (1) multifocal, diffuse, perihilar, or unilateral ground-glass opacity with or without consolidation lacking a specific distribution and are non-rounded or non-peripheral, and (2) few very small ground-glass opacity with a non-rounded and non-peripheral distribution, [19] or atypical findings such as absence of typical or indeterminate features and presence of either: (1) isolated lobar or segmental consolidation without ground-glass opacity, (2) discrete small nodules (centrilobular, “tree-in-bud”), (3) lung cavitation, or (4) smooth interlobular septal thickening with pleural effusion,[19] or negative for pneumonia defined as no CT features to suggest pneumonia.[19]
Results
Demographics and Characteristics of the Study Population
A total of 204 COVID-19 patients were admitted from March to October 2020. The prevalence of T2DM among admitted patients with COVID-19 is 23% (47 out of 204) and 36 of them were included in this study. The medical records of the remaining 11 patients were not available (records that could not be traced and/or retrieved) at the time of data collection, hence they were excluded from the study. The average age of patients with T2DM who were admitted for COVID-19 was 65 ± 11.5 years old and 36.1% of them were over 70 years old. These patients were mostly female (61.1%) and their average body mass index (BMI) was 25.1 ± 3.5 kg/m2. On BMI classification, none were underweight but more than half of the patients were overweight and/or obese. The mean duration of diabetes was 8.4 ± 4.6 years, and 41.7% of them were diagnosed for more than 5 to 10 years. The most common antidiabetic drug used prior to admission was dipeptidyl peptidase 4 (DPP4) inhibitor (58.3%) followed by metformin (52.8%). Other medications used were statins (69.4%) and antihypertensive drugs (83.3%). Hypertension was the leading co-morbidity (83.3%) followed by ASCVD (44.4%) and chronic kidney disease (16.7%). Majority (69%) of the subjects were non-smokers while only 8.3% are current smokers (Table 1).
Table 1. Clinical characteristics of COVID-19 patients with T2DM
Table 1.1
|
|
Mean ± SD |
|
Age (years) |
64.5 ± 11.5 |
|
Body Mass Index (kg/m 2 ) |
25.1 ± 3.5 |
|
Duration of Diabetes Mellitus (years) |
8.4 ± 4.6 |
Table 1.2
|
|
n (%) |
|
Age Group |
|
|
30-40 years old |
1 (2.80) |
|
41-50 years old |
3 (8.30) |
|
51-60 years old |
9 (25.0) |
|
61-70 years old |
10 (27.8) |
|
≥71 years old |
13 (36.1) |
|
Sex |
|
|
Male |
14 (38.9) |
|
Female |
22 (61.1) |
|
Body Mass Index (kg/m2) |
|
|
Underweight (<18.5 kg/m2) |
0 (0) |
|
Normal (18.5 - 22.9 kg/m2) |
10 (27.8) |
|
Overweight (23 - 24.9 kg/m2) |
18 (50.0) |
|
Obese (≥25 kg/m2) |
8 (22.2) |
|
Duration of Diabetes Mellitus (years) |
|
|
Less than 5 years |
8 (22.2) |
|
5 to 10 years |
15 (41.7) |
|
11 to 20 years |
13 (36.1) |
|
Use of Medication |
|
|
A. Oral hypoglycemic agent |
|
|
Metformin |
19 (52.8) |
|
DPP4 Inhibitor |
21 (58.3) |
|
Acarbose |
1 (2.80) |
|
Sulfonylurea |
12 (33.3) |
|
Insulin |
8 (22.2) |
|
Thiazolidinediones |
3 (8.30) |
|
SGLT2 Inhibitors |
2 (5.60) |
|
B. Statins |
25 (69.4) |
|
C. Anti-hypertension drugs |
30 (83.3) |
|
D. Anti-thrombotic drugs |
12 (33.3) |
|
Comorbid Condition |
|
|
Hypertension |
30 (83.3) |
|
Atherosclerotic Cardiovascular Disease |
18 (44.4) |
|
Stroke |
7 (19.4) |
|
Coronary Artery Disease (CAD) |
10 (27.8) |
|
Peripheral Arterial Occlusive Disease (PAOD) |
1 (2.80) |
|
Respiratory Disease |
6 (16.7) |
|
Bronchial Asthma |
2 (5.60) |
|
Tuberculosis |
4 (11.1) |
|
Chronic Kidney Disease (CKD) |
6 (16.7) |
|
Nonalcoholic Fatty Liver Disease (NAFLD) |
3 (8.30) |
|
Neoplasm |
3 (8.30) |
|
Breast Cancer |
1 (2.80) |
|
Thyroid Cancer |
2 (5.60) |
|
Smoking Status |
|
|
Non-Smoker |
25 (69.4) |
|
Former Smoker |
8 (22.2) |
|
Current Smoker |
3 (8.30) |
Clinical Presentation
For the patients with diabetes mellitus and COVID-19 infection, common symptoms were cough (55.6%), fever (50%), dyspnea (36.1%) and fatigue (30.6%). Other symptoms were anorexia (25%), headache (22.2%) and abdominal pain or diarrhea (11.1%). The average duration from exposure to onset of symptoms was 7.8 ± 5 days. The resulting average systolic blood pressure of the subjects was 130 ± 14 mmHg, while the mean diastolic blood pressure was 77.6 ± 8.1 mmHg. The mean heart rate was at 89.7 ± 13.1 beats per minute and the mean respiratory rate was at 24 ± 9 cycles per minute, with 91.7% of the total patients having respiratory rate below 30 cycles per minute. The average oxygen saturation was 92.6% ± 12.6% while the average temperature was 36.9ºC ± 0.7ºC. The average capillary blood glucose (CBG) on admission was 182.4 mg/dL ± 62.8 mg/dL (Table 2).
Table 2. Presenting signs and symptoms of COVID-19 in patients with T2DM
Table 2.1
|
Mean ± SD |
|
| Onset of Symptoms (days) | 7.8 ± 5 |
| Vital Signs | |
| Systolic blood pressure (mmHg) | 129.9 ± 14 |
| Diastolic blood pressure (mmHg) | 77.5 ± 8.1 |
| Heart rate [beats per minute (bpm)] | 89.7 ± 13.1 |
| Respiratory rate [cycles per minute (cpm)] | 24.0 ± 9 |
| Oxygen saturation (%) | 92.6 ± 12.6 |
| Temperature (ºC) | 36.9 ± 0.7 |
| Capillary blood glucose [CBG] (mg/dL) | 182.4 ± 62.8 |
Table 2.2
|
n (%) |
|
| Symptoms |
|
| Fever | 18 (50.0) |
| Sore throat | 3 (8.30) |
| Diarrhea | 4 (11.1) |
| Fatigue | 11 (30.6) |
| Cough | 20 (55.6) |
| Headache | 8 (22.2) |
| Anorexia | 9 (25.0) |
| Anosmia | 0 (0) |
| Dyspnea | 13 (36.1) |
| Myalgia | 3 (8.30) |
| Vomiting | 0 (0) |
| Ageusia | 1 (2.80) |
| Abdominal pain | 4 (11.1) |
| Sign | |
| Respiratory rate, n, % | |
| <30 cpm | 33 (91.7) |
| ≥30 cpm | 3 (8.3) |
Laboratory Parameters
The baseline laboratory results on admission showed that the average hemoglobin, hematocrit, and platelet counts were within normal limits. The average white blood cell (WBC) count was increased with an average of 11.4 x109/uL with a predominance of neutrophils (76.2%). This is notable since lymphocytic predominance is expected in viral infections. Arterial blood gas results showed respiratory alkalosis with a mean pH of 7.5, pCO2 of 30 ± 4 mmHg, pO2 of 99.2 ± 85.3 mmHg, HCO3 of 21.8 ± 3.2 mEq/L, and a mean arterial oxygen saturation of 95.1% ± 3.3%.
Both the mean admission capillary blood glucose (CBG) and fasting CBG were elevated at 182.4 ± 62.8 mg/dL and 153.2 ± 36.1 mg/dL, respectively. The mean pre-prandial CBG and 2-hour postprandial CBG were also elevated at 171.9 ± 32.4 mg/dL and 176.1 ± 35.3 mg/dL. Fasting blood sugar (FBS) in majority of the patients was not done.
The mean HbA1c was 7.9% ± 1.9%. Notably, 36.1% of the patients had an HbA1c between 7% to 8.5% while 27.8% had an HbA1c above 8.5%. The mean estimated glomerular filtration rate (eGFR) of these patients was at 70.9 mL/min/1.73 m2, with 36.1% patients having an eGFR more than 90 mL/min/1.73 m2.
In terms of chest imaging results, 94.4% had characteristic appearance of COVID-19 infection on chest X-ray, while only 5.6% had non-specific chest imaging for COVID-19. Chest CT scan was not done in all subjects (Table 3).
Table 3. Laboratory findings of hospitalized COVID-19 patients with T2DM
Table 3
|
Mean ± SD |
|
| Complete Blood Count | |
| Hemoglobin (g/dL) | 126.1 ± 20.8 |
| Hematocrit (vol.fr.) | 0.4 ± 0.1 |
| WBC Count (x109/L) | 11.4 ± 9.4 |
| Neutrophils (%) | 76.2 ± 21 |
| Lymphocytes (%) | 15.3 ± 10.2 |
| Platelet (x109/L) | 289.2 ± 116.7 |
| Arterial Blood Gas (ABG) | |
| pH | 7.5 ± 0 |
| paCO2 (mmHg) | 30 ± 4 |
| paO2 (mmHg) | 99.2 ± 85.3 |
| HCO3 (mmHg) | 21.8 ± 3.2 |
| O2 Saturation (%) | 95.1 ± 3.3 |
| paO2/FiO2 ratio | 309 ± 124.3 |
| Admission capillary blood glucose (CBG) (mg/dL) | 182.4 ± 62.8 |
| Average CBG during admission (mg/dL) | |
| Fasting (mg/dL) | 153.2 ± 36.1 |
| Pre-prandial (mg/dL) | 171.9 ± 32.4 |
| 2 hours post-prandial (mg/dL) | 176.1 ± 35.3 |
| HbA1c (%) | 7.9 ± 1.9 |
| SGPT (U/L) | 43.5 ± 31.2 |
| SGOT (U/L) | 47.5 ± 24.5 |
| Albumin (g/dL) | 2.9 ± 0.6 |
| Creatinine (mg dL) | 1.2 ± 0.7 |
| eGFR (mL/min/1.73m2) | 70.9 ± 30.8 |
Table 3.2
|
n (%) |
|
| Fasting Plasma Glucose (mg/dL) | |
| <100 mg/dL | 0 (0) |
| 100 to 125 mg/dL | 0 (0) |
| >126 mg/dL | 4 (11.1) |
| Not Done | 32 (88.9) |
| HbA1c | |
| <7% | 13 (36.1) |
| 7%-8.5% | 13 (36.1) |
| >8.5% | 10 (27.8) |
| eGFR (mL/min/1.73 m2) | |
| Below 45 mL/min/1.73 m 2 | 9 (25.0) |
| At least 45 to below 90 mL/min/1.73 m2 | 14 (38.9) |
| More than 90 mL/min/1.73 m2 | 13 (36.1) |
| Imaging | |
| Chest X-ray | |
| Characteristic | 34 (94.4) |
| Nonspecific | 2 (5.6) |
| Negative | 0 (0) |
| Chest CT scan | 0 (0) |
Treatment
The basal-bolus regimen was started on 50% of the hospitalized COVID-19 T2DM patients during admission along with supplemental insulin scale (80.6%). The widely used antidiabetic medication was a DPP4 inhibitor (83.3%). Regarding vasopressor therapy, 16.7% of patients were given norepinephrine. The corticosteroid dexamethasone was given to almost all patients (97.2%), while 5.6% of patients were given methylprednisolone. In terms of oxygen support, 61.1% of patients were given oxygen via high-flow nasal cannula (HFNC) while 27.8% required mechanical ventilation. One-quarter of the patients underwent hemoperfusion (25.0%), while 36.1% received convalescent plasma therapy. Approximately 22.2% of the patients needed blood transfusion (Table 4).
Table 4. Interventions given to hospitalized COVID-19 patients with T2DM.
|
n (%) |
|
| Insulin Therapy |
|
| Basal insulin | 8 (22.2) |
| Basal-bolus insulin | 18 (50.0) |
| Basal insulin + OHA | 0 (0) |
| Bolus insulin only | 1 (2.80) |
| Supplemental scale | 29 (80.6) |
| Oral Hypoglycemic Agents | |
| DPP4 inhibitor | 30 (83.3) |
| Metformin | 2 (5.60) |
| Sulfonylurea | 0 (0) |
| Others (Thiazolidinedione, SGLT2 inhibitor) | 3 (8.30) |
| Vasopressor Therapy | |
| Norepinephrine | 6 (16.7) |
| Dopamine | 1 (2.80) |
| Epinephrine | 1 (2.80) |
| Corticosteroids | |
| Dexamethasone | 35 (97.2) |
| Methylprednisolone | 2 (5.60) |
| Oxygen Support | |
| Nasal cannula | 3 (8.30) |
| High-flow nasal cannula | 22 (61.1) |
| Mechanical ventilation | 10 (27.8) |
| Tracheostomy | 1 (2.80) |
| None | 1 (2.80) |
| Renal Replacement Therapy | 3 (8.30) |
| Hemoperfusion | 9 (25.0) |
| Convalescent plasma therapy | 13 (36.1) |
| Blood transfusion | 8 (22.2) |
Disease Severity and Outcome
Moderate COVID-19 infection occurred in 52.8% of T2DM patients while 27.8% of these patients had critical COVID-19 infection. Of those patients with critical COVID-19 infection, all presented with acute respiratory distress syndrome, with nearly half having concomitant septic shock. Respiratory failure was seen in 27.8% of patients. The average length of hospital stay was 17.5 days. Around 13.9% of these patients had spent more than a month in the hospital. In addition, 25% of patients were admitted in the intensive care unit (ICU) setting. Non-fatal myocardial infarction occurred in 8.3% while non-fatal stroke was seen in 2.8% of patients. The recovery rate of patients with hospitalized T2DM for COVID-19 infection was 86.1%. (Table 5)
Table 5. Disease severity and outcome measures of hospitalized COVID-19 patients with T2DM
|
n (%) |
|
| Disease Severity |
|
| Moderate | 19 (52.8) |
| Severe | 7 (19.4) |
| Critical | 10 (27.8) |
| a. ARDS | 10 (27.8) |
| b. Sepsis | 2 (5.60) |
| c. Septic Shock | 4 (11.1) |
| Respiratory Failure | 10 (27.8) |
| Length of hospital stay | |
| <14 days | 19 (52.8) |
| 14 to 30 days | 12 (33.3) |
| >30 days | 5 (13.9) |
| ICU Admission | 9 (25.0) |
| Morbidity | |
| Non-fatal myocardial infarction | 3 (8.30) |
| Non-fatal stroke | 1 (2.80) |
| Outcome | |
| Died | 5 (13.9) |
| Recovered | 31 (86.1) |
|
Mean ± SD |
|
| Length of hospital stay | 17.5 ± 16.2 |
Risk Factors Associated with Disease Severity and Length of Hospitalization
Established ASCVD is a significant risk factor in the occurrence of severe to critical COVID-19 infection as well as longer length of hospital stay. Adjusting the demographic and clinical characteristics of the subjects, patients with established ASCVD are 5.1 times (95% CI 1.2 to 21.4) more likely to develop severe or critical COVID-19 infection, and more likely to stay in the hospital for more than 14 days as compared to those without established ASCVD. Although not significant, obesity can be a potential risk factor (OR = 3, 0.4 to 22.7) for the development of severe to critical COVID-19 infection as well as longer length of hospital stay. Similarly, although not significant, patients with either a previous stroke (OR = 3.5, 0.6 to 21.4) or those with existing coronary artery disease (OR = 3.7, 0.8 to 17.9) may have the potential risk to develop severe to critical disease. Additionally, an HbA1c level of more than 8.5% turns out to be a potential risk (OR = 3.7, 0.6 to 21.6) for severe to critical disease. As to the length of hospital stay, results reveal that patients with diabetes and concomitant coronary artery disease are 7.6 times (95% CI 1.3 to 43.4) more likely to stay longer (more than 14 days) as compared to those without existing coronary artery disease (Table 6).
Table 6. Univariable logistic regression for risk factors associated with disease severity and length of hospitalization in T2DM patients with COVID-19
|
Severity (Mild-Moderate vs Severe-Critical) |
LOS (<14 days vs >/=14 days) |
|||
|
OR (95% CI) |
p-value |
OR (95% CI) |
p-value |
|
| Age Group, n, % |
|
|
|
|
| Below 60 years old |
Reference |
Reference |
||
| 60 to 70 years old |
0.7 (0.2-2.6) |
0.5504 ns |
1.1 (0.3-4.2) |
0.9231 ns |
| ≥71 years old |
|
|
|
|
| Sex, n, % |
|
|
|
|
| Male |
0.8 (0.2-2.9) |
0.6759 ns |
0.5 (0.1-1.8) |
0.2734 ns |
| Female |
Reference |
Reference |
||
|
BMI Classification (kg/m2), n, % |
|
|
|
|
| Underweight (<18.5) |
- |
- |
- |
- |
| Normal (18.5 - 22.9) |
Reference |
Reference |
||
| Overweight (23 - 24.9) |
0.5 (0.1-2.4) |
0.3899 ns |
1.2 (0.2-5.8) |
0.8200 ns |
| Obese (≥25) |
3 (0.4-22.7) |
0.2875 ns |
2.5 (0.4-16.9) |
0.3472 ns |
| Duration of Diabetes Mellitus, n, % |
|
|
|
|
| Less than 5 years |
Reference |
Reference |
||
| 5 to 10 years |
0.5 (0.1-3.) |
0.4716 ns |
0.3 (0.0-1.9) |
0.2025 ns |
| 11 to 20 years |
0.4 (0.1-2.3) |
0.2897 ns |
0.1 (0-1.1) |
0.2025 ns |
| >20 years |
- |
- |
- |
- |
| Use of Medication, n, % |
|
|
|
|
| Metformin |
1.6 (0.4-5.9) |
0.4929 ns |
1 (0.3-3.8) |
0.9852 ns |
| DPP4 inhibitor |
0.7 (0.2-2.5) |
0.5356 ns |
0.3 (0.1-1.0) |
0.0532 ns |
| Acarbose |
- |
0.4722 ns |
- |
0.4722 ns |
| Sulfonylurea |
0.4 (0.1-1.8) |
0.2430 ns |
0.2 (0.1-1.1) |
0.0675 ns |
| Insulin |
1.2 (0.2-5.6) |
0.8584 ns |
2.2 (0.4-11.2) |
0.3326 ns |
| Thiazolidinedione |
0.5 (0-6.4) |
0.6194 ns |
- |
0.0952 ns |
| SGLT2 inhibitor |
- |
0.2159 ns |
1.1 (0.1-19.5) |
0.9355 ns |
| Statin |
1.1 (0.3-4.6) |
0.8879 ns |
0.4 (0.1-1.7) |
0.197 ns |
| Antihypertensive drug |
2 (0.3-12.6) |
0.4608 ns |
0.4 (0.1-2.4) |
0.307 ns |
| Anti-thrombotic |
2 (0.5-8) |
0.3481 ns |
2 (0.5-8) |
0.3481 ns |
| Comorbid Condition, n, % |
|
|
|
|
| Hypertension |
2 (0.3-12.6) |
0.4608 ns |
0.4 (0.1-2.4) |
0.307 ns |
| ASCVD |
5.1 (1.2-21.4) |
0.0245* |
5.1 (1.2-21.4) |
0.0245* |
| Stroke |
3.5 (0.6-21.4) |
0.1682 ns |
1.6 (0.3-8.7) |
0.5601 ns |
| Coronary Artery Disease |
3.7 (0.8-17.9) |
0.0993 ns |
7.6 (1.3-43.4) |
0.0233* |
| Peripheral Arterial Occlusive Disease |
- |
1.000 ns |
- |
1.000 ns |
| Respiratory Disease |
0.2 (0.0-1.7) |
0.13133 ns |
1.1 (0.2-6.6) |
0.8814 ns |
| Asthma |
- |
0.4873 ns |
- |
0.2159 ns |
| COPD |
- |
- |
- |
- |
| Tuberculosis |
0.3 (0-3.5) |
0.3630 ns |
0.3 (0-3.5) |
0.3630 ns |
| Chronic Kidney Disease |
0.5 (0.1-3.2) |
0.4608 ns |
1.1 (0.2-6.6) |
0.8814 ns |
| Non-alcoholic Fatty Liver |
- |
0.2310 ns |
0.5 (0.0-6.4) |
0.6194 ns |
| Neoplasm |
- |
0.2310 ns |
2.4 (0.2-29.1) |
0.4919 ns |
| Breast Cancer |
- |
1.0000 ns |
- |
0.4722 ns |
| Thyroid Cancer |
- |
- |
- |
- |
| Smoking Status, n, % |
|
|
|
|
| Non-Smoker |
Reference |
Reference |
||
| Previous Smoker |
0.7 (0.1-3.3) |
0.6050 ns |
0.3 (0.0-1.6) |
0.1412 ns |
| Current Smoker |
2.2 (0.2-27.1) |
0.5485 ns |
0.4 (0.0-4.9) |
0.4687 ns |
| HbA1c |
|
|
|
|
| <7% |
Reference |
Reference |
||
| 7%-8.5% |
1 (0.2-4.9) |
1.0000 ns |
1 (0.2-4.9) |
1.0000 ns |
| >8.5% |
3.7 (0.6-21.6) |
0.1411 ns |
1.2 (0.2-6.1) |
0.8548 ns |
*s- Significant; ns -not significant
Risk Factors Associated with ICU Admission, Morbidity and Mortality
The intake of statins prior to admission was a significant risk factor for ICU admission (p-value = 0.0341). Specifically, those patients on statins were more likely to be admitted in the ICU as compared to those who were not taking it. The odds ratio in prior statin use is undefined since all patients who were admitted in the ICU were using statins prior to admission. When prior statin use was subdivided into those patients with and without pre-existing ASCVD, though not significant, the prior use of statins in patients with pre-existing ASCVD have the potential risk for ICU admission (OR = 2.0, 0.4 to 10.9), as compared to those patients without pre-existing ASCVD. Though not significant, the presence of a previous stroke (OR = 2.9, 0.5 to 16.5) or coronary artery disease (OR = 2.8, 0.6 to 13.8) were potential risk factors of ICU admission. None of the other clinical factors turned out to be a significant risk for morbidity and mortality. However, those who were taking thiazolidinediones prior to admission had the potential risk for morbidity (eg, non-fatal myocardial infarction, non-fatal stroke) during hospitalization, although it was not significant (OR = 7.8, 0.5 to 126.7). Other factors that may be a potential risk for morbidity during hospitalization for COVID-19 are intake of anti-thrombotic drugs (OR = 4.6, 0.4 to 56.8), having a previous stroke (OR = 11.2, 0.8 to 148.1) and having existing coronary artery disease (OR = 6.3, 0.5 to 78.4). For mortality, obesity may be a potential risk factor (OR = 5.4, 0.4 to 66.7) as well as the intake of SGLT2 inhibitors (OR=7.5,0.4 to 145). An HbA1c level above 8.5% was also seen as a potential risk factor for mortality (OR = 5.1, 0.4 to 59.5) (Table 7).
Table 7. Univariable logistic regression for risk factors associated with ICU admission, morbidity, and mortality in T2 DM patients with COVID-19
|
ICU Admission |
Morbidity |
Mortality |
||||
|
OR (95% CI) |
p-value |
OR (95% CI) |
p-value |
OR (95% CI) |
p-value |
|
| Age Group, n, % |
|
|
|
|
|
|
| Below 60 years old |
Reference |
Reference |
Reference |
|||
| 60 to 70 years old |
1.2 (0.2-5.8) |
0.8413 ns |
0.3 (0-3.1) |
0.2785 ns |
- |
0.1363 ns |
| ≥71 years old |
|
|
|
|
|
|
| Sex, n, % |
|
|
|
|
|
|
| Male |
1.4 (0.3-6.3) |
0.6935 ns |
- |
0.2667 ns |
- |
0.1336 ns |
| Female |
Reference |
Reference |
Reference |
|||
| BMI Classification, kg/m2 , n, % |
|
|
|
|
|
|
|
Underweight (<18.5) |
- |
- |
- |
- |
- |
- |
|
Normal (18.5 - 22.9) |
Reference |
Reference |
Reference |
|||
|
Overweight (23 - 24.9) |
0.5 (0.1-2.9) |
0.4155 ns |
- |
0.5840 ns |
0.5 (0-9.5) |
0.6659 ns |
| Obese (≥25) |
1.4 (0.2-10.0) |
0.7377 ns |
- |
0.5840 ns |
5.4 (0.4-66.7) |
0.1885 ns |
| Duration of Diabetes Mellitus (years), n, % |
|
|
|
|
|
|
| Less than 5 years |
Reference |
Reference |
Reference |
|||
| 5 to 10 years |
2.5 (0.2-27.7) |
0.4431 ns |
- |
0.4265 ns |
0.5 (0.0-9.2) |
0.6414 ns |
| 11 to 20 years |
3.1 (0.3-34.4) |
0.3547 ns |
- |
0.4265 ns |
2.1 (0.2-24.6) |
0.5545 ns |
| >20 years |
- |
- |
- |
- |
- |
- |
| Use of Medication, n, % |
|
|
|
|
|
|
| Metformin |
0.6 (0.1-2.9) |
0.5645 ns |
0.4 (0-5.1) |
0.4919 ns |
1.4 (0.2-9.6) |
0.7287 ns |
| DPP4 inhibitor |
1.6 (0.3-7.8) |
0.5599 ns |
0.3 (0-4) |
0.3782 ns |
3.3 (0.3-32.9) |
0.3102 ns |
| Acarbose |
- |
0.2500 ns |
- |
1.0000 ns |
- |
0.1389 ns |
| Sulfonylurea |
1.9 (4-9) |
0.4178 ns |
- |
0.5361 ns |
1.4 (0.2-9.8) |
0.7341 ns |
| Insulin |
1.0 (0.2-6.1) |
1.0000 ns |
1.9 (0.1-23.6) |
0.6331 ns |
0.9 (0.1-9) |
0.8976 ns |
| Thiazolidinedione |
- |
0.5576 ns |
7.8 (0.5-126.7) |
0.1509 ns |
- |
1.0000 ns |
| SGLT2 inhibitor |
3.3 (0.2-58.1) |
0.4229 ns |
- |
1.0000 ns |
7.5 (0.4-145) |
0.1824 ns |
| Statin |
∞- |
0.0341* |
0.9 (0.1-10.7) |
0.9132 ns |
1.9 (0.2-19.3) |
0.5857 ns |
| A. Statin users with pre-existing ASCVD |
2.0 (0.4-10.9) |
0.4235 ns |
- |
- |
- |
- |
| B. Statin users without pre-existing ASCVD |
Reference |
- |
- |
- |
- |
|
| Antihypertensives |
- |
0.3026 ns |
- |
1.0000 ns |
0.8 (0.1-8.4) |
0.8297 ns |
| Anti-thrombotic drugs |
1.9 (0.4-9) |
0.4178 ns |
4.6 (0.4-56.8) |
0.2339 ns |
1.4 (0.2-9.8) |
0.7341 ns |
| Comorbid Condition, n, % |
|
|
|
|
|
|
| Hypertension |
- |
0.3026 ns |
- |
1.0000 ns |
- |
1.0000 ns |
| ASCVD |
3.4 (0.7-16.7) |
0.1316 ns |
- |
0.0784 ns |
2.1 (0.3 to 14.3) |
0.4571 ns |
| Stroke |
2.9 (0.5-16.5) |
0.2358 ns |
11.2 (0.8-148.1) |
0.0667 ns |
3.5 (0.5-26.4) |
0.2298 ns |
| CAD |
2.8 (0.6-13.8) |
0.2065 ns |
6.3 (0.5-78.4) |
0.1555 ns |
0.6 (0.1-6.2) |
0.6780 ns |
| PAOD |
- |
1.0000 ns |
- |
1.0000 ns |
- |
1.0000 ns |
| Respiratory Disease |
0.6 (0.1-5.5) |
0.6096 ns |
- |
1.0000 ns |
1.3 (0.2-14.2) |
0.8297 ns |
| Asthma |
- |
1.0000 ns |
- |
1.0000 ns |
- |
1.0000 ns |
| COPD |
- |
- |
- |
- |
- |
- |
| Bronchiectasis |
- |
- |
- |
- |
- |
- |
| Tuberculosis |
- |
1.0000 ns |
- |
1.0000 ns |
2.3 (0.2-28.3) |
0.5055 ns |
| CKD |
0.6 (0.1-5.5) |
0.6096 ns |
2.8 (0.2-37.0) |
0.4345 ns |
- |
0.5638 ns |
| Fatty liver |
- |
0.5576 ns |
- |
1.0000 ns |
- |
1.0000 ns |
| Neoplasm |
- |
0.5576 ns |
- |
1.0000 ns |
- |
1.0000 ns |
| Breast Cancer |
- |
1.0000 ns |
- |
1.0000 ns |
- |
1.0000 ns |
| Thyroid Cancer |
- |
- |
- |
- |
- |
- |
| Smoking Status, n, % |
|
|
|
|
|
|
| Non-Smoker |
Reference |
Reference |
Reference |
|||
| Former Smoker |
- |
0.5765 ns |
- |
1.0000 ns |
- |
1.0000 ns |
| Current Smoker |
- |
0.5765 ns |
- |
1.0000 ns |
- |
1.0000 ns |
| Hb1ac |
|
|
|
|
|
|
| <7% |
Reference |
Reference |
Reference |
|||
| 7%-8.5% |
2.4 (0.4-16.5) |
0.3596 ns |
1 (0.1-17.9) |
1.0000 ns |
1 (0.1-17.9) |
1.0000 ns |
| >8.5% |
2.4 (0.3-17.9) |
0.4065 ns |
1.3 (0.1-24.3) |
0.846 ns |
5.1 (0.4-59.5) |
0.1897 ns |
*s- significant; ns- not significant;
BMI – Body Mass Index;
Discussion
Our study had shown that the prevalence rate of T2DM in patients with COVID-19 infection is 23%, which is slightly higher than that reported by Abdi, et al. (10-20%),[3] but is in congruence with the prevalence rate between 8% to 37% reported in several international research articles.[17,27] The average age of our patients was 65 ± 11.5 years old and 36.1% of them were over 70 years old, which was different in the study population in one center in South Korea where patients enrolled were relatively young (average age 37.6 years old).[20] Majority of our patients had cough and fever while a subset experienced fatigue and dyspnea. The mean duration of onset of these symptoms was around eight days. The characteristic appearance of COVID-19 infection on chest X-ray such as bilateral “patchy” and/or “confluent, bandlike” ground glass opacity or consolidation in a peripheral and mid-to-lower lung zone distribution [26] was seen in 94.4% of our patients. Only two patients had new-onset diabetes while the rest had diabetes for more than 5 years. Half of our study population was overweight and 22% obese. In the influenza pandemic of 2009, one study reported that obesity was shown to be associated with increased risk of mortality, and the need for hospitalization and ICU admission and ventilator support.[23] Obesity was also found to be a potential risk factor for severe disease and in-hospital mortality. Several meta-analyses confirm this finding in our study, indicating that obesity is an independent risk and prognostic factor for severe COVID-19 infection and may increase the risk of hospitalization, ICU admission, need for mechanical ventilation and even death. [27, 28] The underlying mechanism by which obesity increases the risk of severe COVID-19 infection remains unknown but may be explained by the role of combined adipose tissue-mediated immune and metabolic dysfunction influencing COVID-19 prognosis. Muniyappa, et al. reported the five main possible mechanisms that may underlie increased susceptibility to COVID-19 in patients with diabetes mellitus: (i) greater affinity of COVID-19 for cellular binding and entry; (ii) reduced viral clearance; (iii) reduced T-cell function; (iv) coexistent cardiovascular disease; and (v) susceptibility to cytokine storm and hyper-inflammation.[29] An explanation for the increased rate of hospitalization of patients with diabetes mellitus after the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV) epidemic was the reduced usage of regular effective care by patients with diabetes mellitus. With these lessons learned from the past and the continuous knowledge we seek in the present pandemic, regular effective care of patients with T2DM during this pandemic was stepped up in our medical center by using telemedicine outpatient consultation and massive information campaign through bulletin boards, poster, and social media. This could have contributed to the decreased number of COVID-19 infections in patients with diabetes mellitus and the small sample size in our center. Patients with mild COVID-19 infection were not admitted but advised for home quarantine.
Diabetes mellitus represents an important independent risk factor for COVID-19 infection as well as adverse outcomes. The prevailing glycemic control contributes to this risk. As shown in one multi-center study involving more than 7,300 cases of COVID-19 with pre-existing T2DM, those hospitalized cases with well-controlled glycemia had markedly lower mortality rates than cases with poor glycemia (defined by the upper limit of glycemic variability exceeding 10 mmol/l), with a hazard ratio of 0.14.[24] On the other hand, patients with diabetes mellitus with inadequate glycemic control and COVID-19 infection have a higher risk of infection and an increased likelihood of poorer clinical outcomes, as compared to patients with good glycemic control.[24,30] The impaired T-cell mediated immune response and uncontrolled chronic hyperglycemia lead to a higher propensity for infections and development of worse complications.[7] On admission, the in-hospital average capillary blood glucose levels of our patients were less than 180 mg/dL, which reflect adequate glucose control despite the COVID-19 infection. But one can argue that the presence of anorexia in these patients can contribute to lower plasma glucose levels. The good glycemic control may explain the recovery rate of more than 80% for our enrolled patients.
Metformin is the first line of therapy for T2DM, so it is not surprising that more than 50% of our study population are on this drug before admission. Because of its potential side effects of lactic acidosis, increased risk of renal, cardiac, and liver impairment, hypotension and acute illness, the NICE guidelines recommend temporary discontinuation of metformin therapy in COVID-19 infection. Although angiotensin-converting enzyme 2 (ACE2) is the cellular receptor for COVID-19 and SARS-CoV, it appears that the cellular entry of COVID-19 is independent from the DPP-4 receptor.[31, 35] DPP-4 inhibitor therapies are therefore allowed in patients with diabetes mellitus and COVID-19 infection, which was continued and maintained during admission in some of our patients. Thiazolidinediones are not recommended for T2DM during this pandemic because of its adverse effects of sodium retention, anemia, and congestive heart failure.[35] SGLT2 inhibitor therapies can also increase the risk of diabetic ketoacidosis, especially in older patients, thus temporary discontinuation of this therapy in any acute illness including COVID-19 is a precautionary measure. On admission, only 22% of our patients were previously on insulin and the rest were on oral antidiabetic agents. In patients with diabetes mellitus, any infection can worsen glycemic control through stress because of enhanced cortisol release. This was further exacerbated in COVID-19 infection because the pathway for treatment includes the use of exogenous glucocorticoid therapy. These patients on oral antidiabetic agents were then shifted to basal-bolus insulin regimen with glucose monitoring. Optimal glycemic management often requires frequent adjustments to insulin-based therapies. Management was particularly challenging during this pandemic with many healthcare staff stepping outside of their usual working practices, wearing personal protective equipment which can hamper their work, some staff less familiar with the logistics and practicalities of conversion and ongoing management of intravenous insulin-based therapies.
The co-existence of established ASCVD (coronary artery disease, cerebrovascular disease, and peripheral arterial occlusive disease) in patients with T2DM and COVID-19 infection increased the likelihood of severe COVID-19 infection five-fold compared with patients without established ASCVD. These conditions may also increase the risk for morbidity and in-hospital mortality. De Almeida-Pittito, et al. [21] also reported the same finding that pre-existing CVD was the greatest risk factor for COVID-19 severity and mortality. This association between DM, ASCVD and COVID-19 infection was explained by the effects of oxidative stress, inflammation and prothrombotic status. [7,28] These cause oxidative damage and vascular remodeling, thus increasing the risk for severe disease and mortality.[28]
Interestingly, it was found in this study that patients who used statins prior to admission for COVID-19 disease were more likely to be admitted in the ICU compared to those patients who are not taking it.[32]The beneficial role of statins in patients with diabetes mellitus and cardiovascular disease is attributed to its pleiotropic, anti-inflammatory, and immunomodulatory effects, accounting for its recommendation and widespread use.[33] In an observational study done by Mitachhione, et al., [34] however, they reported that statin users before admission showed more comorbidities and more severe COVID-19 infection, which was consistent with the findings in our study. Prior statins use and pre-existing ASCVD may potentially increase the risk of admission in the ICU, as compared to those without ASCVD. This trend toward a poor outcome in patients with pre-existing ASCVD who were on statin therapy may be driven by the presence of pre-existing ASCVD in these patients.
Prior use of thiazolidinediones and SGLT2 inhibitors have the potential risk for morbidity (e.g., non-fatal myocardial infarction, non-fatal stroke). This is supported by the fact that these medications both enhance the expression of ACE2, the cell receptor for severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2). [35] As these medications may contribute to poor clinical outcomes in COVID-19,[36] their use may need to be re-evaluated in patients with diabetes who develop COVID-19 infection.
The use of anti-thrombotic therapy (namely, aspirin, clopidogrel) also has the potential risk for morbidity. This finding may be supported by a study done by Ho, et al. [20] stating that patients with prior anticoagulation or antiplatelet use had an increased risk of severe clinical outcomes and ICU stay. Moreover, a higher mortality risk was noted in patients with underlying obesity and hypertension.[20] These findings may be influenced by the increased risk of certain comorbidities such as CVD in patients on these medications, compared to those who are not taking them. Some medical experts have advocated the empiric use of anticoagulation in COVID-19 infection. Since COVID-19 is an evolving infection, more studies are needed to elucidate the use of anti-thrombotic drugs in COVID-19.
Conclusion
Patients with T2DM are more vulnerable to COVID-19 infection. T2DM and established ASCVD increase the likelihood of severe COVID-19 disease as well as having a length of hospital stay of more than 14 days. Other potential risk factors that may contribute to disease severity and prognosis among patients with diabetes mellitus include obesity, poor glycemic control (HbA1c >8.5%), prior use of thiazolidinediones, anti-thrombotic drugs and SGLT2 inhibitors. Increased recognition and prompt treatment led to a favorable recovery rate.
Limitation of the Study
The limitations of this study are as follows:
This study only involved review of a patient’s hospital record (retrospective study) during his/her previous admission, missing data and records may have caused a selection and information bias. The short duration of the study may be the reason why included subjects were mostly the elderly population, a vulnerable group of individuals. There was a limited number of subjects since this study is a single-center study with a small sample size.
Nonetheless, despite these limitations, the findings in this study would prove beneficial in improving scientific knowledge as well as social awareness of this highly virulent and evolving COVID-19 infection.
Recommendations
The following are recommended for future research studies:
A prospective observational study, multi-center, involving both public and private medical centers, and with longer duration of recruitment to identify the clinical profile and outcomes of COVID-19 patients with T2DM.
Conflict of Interest
The primary investigator and co-investigators in this study have no conflict of interest in any form, whether it be financial, familial, or proprietary considerations, in the conduct of this study.
- Nanditha A, Ma RCW, Ramachandran A, Snehalatha C, Chan JCN, Chia KS, et al. Diabetes in Asia and the Pacific: Implications for the global epidemic. Diabetes Care [Internet]. 2016;39(3):472–85. Available from: http://dx.doi.org/10.2337/dc15-1536
- International Diabetes Federation (IDF) Atlas. 9th ed. Brussels, Belgium: International Diabetes Federation; 2019.
- Abdi A, Jalilian M, Sarbarzeh PA, Vlaisavljevic Z. Diabetes and COVID-19: A systematic review on the current evidence. Diabetes Res Clin Pract [Internet]. 2020;166(108347):108347. Available from: http://dx.doi.org/10.1016/j.diabres.2020.108347
- World Health Organization (WHO) Coronavirus Disease (COVID-19) Dashboard [Internet]. World Health Organization. [cited 2020]. Available from: https://covid19.who.int/?gclid=CjwKCAjwiOv7BRBREiwAXHbv3Nc7ib5xPDvo3St2jZ8x7ndqDnEv5rplPzuTZoh5MihUdQ31wOT10RoCkOYQAvD_BwE.
- Apicella M, Campopiano MC, Mantuano M, Mazoni L, Coppelli A, Del Prato S. COVID-19 in people with diabetes: understanding the reasons for worse outcomes. Lancet Diabetes Endocrinol [Internet]. 2020;8(9):782–92. Available from: http://dx.doi.org/10.1016/S2213-8587(20)30238-2
- Gupta R, Hussain A, Misra A. Diabetes and COVID-19: evidence, status and unanswered research questions. Eur J Clin Nutr [Internet]. 2020;74(6):1–7. Available from: http://dx.doi.org/10.1038/s41430-020-0652-1
- Hussain A, Bhowmik B, do Vale Moreira NC. COVID-19 and diabetes: Knowledge in progress. Diabetes Res Clin Pract [Internet]. 2020;162(108142):108142. Available from: http://dx.doi.org/10.1016/j.diabres.2020.108142
- Kumar A, Arora A, Sharma P, Anikhindi SA, Bansal N, Singla V, et al. Is diabetes mellitus associated with mortality and severity of COVID-19? A meta-analysis. Diabetes Metab Syndr [Internet]. 2020;14(4):535–45. Available from: http://dx.doi.org/10.1016/j.dsx.2020.04.044
- Li H, Tian S, Chen T, Cui Z, Shi N, Zhong X, et al. Newly diagnosed diabetes is associated with a higher risk of mortality than known diabetes in hospitalized patients with COVID-19. Diabetes Obes Metab [Internet]. 2020;22(10):1897–906. Available from: http://dx.doi.org/10.1111/dom.14099
- Shi Q, Zhang X, Jiang F, Zhang X, Bimu C, Feng J, et al. Clinical characteristics, and risk factors for mortality of COVID-19 patients with diabetes in Wuhan, China: A two-center, retrospective study [Internet]. American Diabetes Association. 2020. Available from: http://dx.doi.org/10.2337/figshare.12210008
- Salva EP, Villarama JB, Lopez EB, Sayo AR, Villanueva AMG, Edwards T, et al. Epidemiological and clinical characteristics of patients with suspected COVID-19 admitted in Metro Manila, Philippines. Trop Med Health [Internet]. 2020;48(1):51. Available from: http://dx.doi.org/10.1186/s41182-020-00241-8
- Buenaventura RD, Ho JB, Lapid MI. COVID-19 and mental health of older adults in the Philippines: a perspective from a developing country. Int Psychogeriatr [Internet]. 2020;30:1–5. Available from: http://dx.doi.org/10.1017/S0141610220000757
- Elvira Arcellana A, Jimeno C. Challenges, and opportunities for diabetes care in the Philippines in the time of the COVID-19 pandemic. J ASEAN Fed Endocr Soc [Internet]. 2020;35(1):55–7. Available from: http://dx.doi.org/10.15605/jafes.035.01.04
- Gamble A, Pham Q, Goyal S, Cafazzo JA. The challenges of COVID-19 for people living with diabetes: Considerations for digital health. JMIR Diabetes [Internet]. 2020;5(2):e19581. Available from: http://dx.doi.org/10.2196/19581
- World Health Organization. Regional Office for the Western Pacific. The Asia-Pacific perspective: redefining obesity and its treatment [Internet]. Sydney: Health Communications Australia; 2000 [cited 2023]. Available from: https://iris.who.int/handle/10665/206936
- Singh AK, Singh R. Hyperglycemia without diabetes and new-onset diabetes are both associated with poorer outcomes in COVID-19. Diabetes Res Clin Pract [Internet]. 2020;167(108382):108382. Available from: http://dx.doi.org/10.1016/j.diabres.2020.108382
- Alkundi A, Mahmoud I, Musa A, Naveed S, Alshawwaf M. Clinical characteristics, and outcomes of COVID-19 hospitalized patients with diabetes in the United Kingdom: A retrospective single centre study. Diabetes Res Clin Pract [Internet]. 2020;165(108263):108263. Available from: http://dx.doi.org/10.1016/j.diabres.2020.108263
- World Health Organization. Clinical management of COVID-19: interim guidance, 27 May 2020 [Internet]. World Health Organization; 2020 [cited 2023]. Available from: https://iris.who.int/handle/10665/332196
- Simpson S, Kay FU, Abbara S, Bhalla S, Chung JH, Chung M, et al. Radiological society of North America expert consensus document on reporting chest CT findings related to COVID-19: Endorsed by the Society of Thoracic Radiology, the American College of Radiology, and RSNA. Radiol Cardiothorac Imaging [Internet]. 2020;2(2):e200152. Available from: http://dx.doi.org/10.1148/ryct.2020200152
- Chang MC, Park Y-K, Kim B-O, Park D. Risk factors for disease progression in COVID-19 patients. BMC Infect Dis [Internet]. 2020;20(1):445. Available from: http://dx.doi.org/10.1186/s12879-020-05144-x
- de Almeida-Pititto B, Dualib PM, Zajdenverg L, Dantas JR, de Souza FD, Rodacki M, et al. Severity and mortality of COVID 19 in patients with diabetes, hypertension, and cardiovascular disease: a meta-analysis. Diabetol Metab Syndr [Internet]. 2020;12(1):75. Available from: http://dx.doi.org/10.1186/s13098-020-00586-4
- Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension [Internet]. 2018;71(6):e13–115. Available from: http://dx.doi.org/10.1161/HYP.0000000000000065
- Barber TM. COVID-19 and diabetes mellitus: implications for prognosis and clinical management. Expert Rev Endocrinol Metab [Internet]. 2020;15(4):227–36. Available from: http://dx.doi.org/10.1080/17446651.2020.1774360
- Zhu L, She Z-G, Cheng X, Qin J-J, Zhang X-J, Cai J, et al. Association of blood glucose control and outcomes in patients with COVID-19 and pre-existing type 2 diabetes. Cell Metab [Internet]. 2020;31(6):1068-1077.e3. Available from: http://dx.doi.org/10.1016/j.cmet.2020.04.021
- American Diabetes Association. 2. Classification and diagnosis of diabetes: Standards of medical care in diabetes-2020. Diabetes Care [Internet]. 2020;43(Suppl 1):S14–31. Available from: http://dx.doi.org/10.2337/dc20-S002
- Smith DL, Grenier J-P, Batte C, Spieler B. A characteristic chest radiographic pattern in the setting of the COVID-19 pandemic. Radiol Cardiothorac Imaging [Internet]. 2020;2(5):e200280. Available from: http://dx.doi.org/10.1148/ryct.2020200280
- Huang Y, Lu Y, Huang Y-M, Wang M, Ling W, Sui Y, et al. Obesity in patients with COVID-19: a systematic review and meta-analysis. Metabolism [Internet]. 2020;113(154378):154378. Available from: http://dx.doi.org/10.1016/j.metabol.2020.154378
- Tamara A, Tahapary DL. Obesity as a predictor for a poor prognosis of COVID-19: A systematic review. Diabetes Metab Syndr [Internet]. 2020;14(4):655–9. Available from: http://dx.doi.org/10.1016/j.dsx.2020.05.020
- Muniyappa R, Gubbi S. COVID-19 pandemic, corona viruses, and diabetes mellitus. Am J Physiol Endocrinol Metab. 2020;E736–41.
- Gupta R, Ghosh A, Singh AK, Misra A. Clinical considerations for patients with diabetes in times of COVID-19 epidemic. Diabetes Metab Syndr [Internet]. 2020;14(3):211–2. Available from: http://dx.doi.org/10.1016/j.dsx.2020.03.002
- Ni W, Yang X, Yang D, Bao J, Li R, Xiao Y, et al. Role of angiotensin-converting enzyme 2 (ACE2) in COVID-19. Crit Care [Internet]. 2020;24(1):422. Available from: http://dx.doi.org/10.1186/s13054-020-03120-0
- Saeed O, Castagna F, Agalliu I, Xue X, Patel SR, Rochlani Y, et al. Statin use and in-hospital mortality in patients with diabetes mellitus and COVID-19. J Am Heart Assoc [Internet]. 2020;9(24):e018475. Available from: http://dx.doi.org/10.1161/JAHA.120.018475
- Tan WYT, Young BE, Lye DC, Chew DEK, Dalan R. Statin use is associated with lower disease severity in COVID-19 infection. Sci Rep [Internet]. 2020;10(1):17458. Available from: http://dx.doi.org/10.1038/s41598-020-74492-0
- Mitacchione G, Schiavone M, Curnis A, Arca M, Antinori S, Gasperetti A, et al. Impact of prior statin use on clinical outcomes in COVID-19 patients: data from tertiary referral hospitals during COVID-19 pandemic in Italy. J Clin Lipidol [Internet]. 2021;15(1):68–78. Available from: http://dx.doi.org/10.1016/j.jacl.2020.12.008
- Reshad RAI, Riana SH, Chowdhury MA-B, Moin AT, Miah F, Sarkar B, et al. Diabetes in COVID-19 patients: challenges and possible management strategies. Egypt J Bronchol [Internet]. 2021;15(1). Available from: http://dx.doi.org/10.1186/s43168-021-00099-2
![]() Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0
International License, which permits use, share — copy and redistribute the material in any medium or format,
adapt — remix, transform, and build upon the material, as long as you give appropriate credit,
provide a link to the license, and indicate if changes were made. You may do so in any reasonable manner,
but not in any way that suggests the licensor endorses you or your use. You may not use the material for
commercial purposes. If you remix, transform, or build upon the material, you must distribute your
contributions under the same license as the original. You may not apply legal terms or technological
measures that legally restrict others from doing anything the license permits. The images or other
third party material in this article are included in the article’s Creative Commons license, unless indicated
otherwise in a credit line to the material. If material is not included in the article’s Creative Commons
license and your intended use is not permitted by statutory regulation or exceeds the permitted use,
you will need to obtain permission directly from the copyright holder. To view a copy of this license,
visit https://creativecommons.org/licenses/by-nc-sa/4.0/.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0
International License, which permits use, share — copy and redistribute the material in any medium or format,
adapt — remix, transform, and build upon the material, as long as you give appropriate credit,
provide a link to the license, and indicate if changes were made. You may do so in any reasonable manner,
but not in any way that suggests the licensor endorses you or your use. You may not use the material for
commercial purposes. If you remix, transform, or build upon the material, you must distribute your
contributions under the same license as the original. You may not apply legal terms or technological
measures that legally restrict others from doing anything the license permits. The images or other
third party material in this article are included in the article’s Creative Commons license, unless indicated
otherwise in a credit line to the material. If material is not included in the article’s Creative Commons
license and your intended use is not permitted by statutory regulation or exceeds the permitted use,
you will need to obtain permission directly from the copyright holder. To view a copy of this license,
visit https://creativecommons.org/licenses/by-nc-sa/4.0/.