Factors Associated with Insulin Usage in Patients with Gestational Diabetes Mellitus Given Antenatal Corticosteroid
Ria Breneli A. Sumampong-Timpac, Maria Honolina S. Gomez
Apr 2025 DOI 10.35460/2546-1621.2024-0012

Introduction
The American Congress of Obstetricians and Gynecologists (ACOG) recommends the administration of antenatal steroids to patients at risk of preterm delivery between 24- and 36-weeks age of gestation. The recommendation is based on its benefit in decreasing the risk of respiratory distress syndrome, intraventricular hemorrhage and neonatal death. [1-3] In women with diabetes, this need is even more pronounced. Antenatal women with diabetes are at higher risk of experiencing various obstetric and medical complications. Fetal lung maturity is delayed in pregnancies where euglycemia is not achieved. These facts imply that antenatal corticosteroids (ACS) may be required to improve neonatal survival in preterm pregnancies complicated by diabetes. Women with gestational diabetes were more likely (odds ratio 1.21; 95% confidence interval 1.05-1.40) to receive ACS in a study conducted in British Columbia, Canada.[4]
The Fifth International Workshop Conference on Gestational Diabetes Mellitus (2007) recommendation acknowledges that the frequency of preterm delivery is higher in women with untreated gestational diabetes mellitus (GDM). It recommends following normal indications for the use of ACS, albeit with “intensified monitoring of maternal glucose levels” and “temporary addition or increase of insulin doses”.[5] Furthermore, the National Institute of Health and Clinical Excellence (NICE) published clinical guideline for diabetes in pregnancy that states that diabetes should not be considered a contra-indication to ACS.[6]
Steroid use should warrant more aggressive screening for GDM, above and beyond routine recommendations.[7] Antenatal steroid administration may worsen glycemic profile primarily in those with overt diabetes mellitus or GDM through its overall diabetogenic effects. This drug with all its benefit on the fetus poses a challenge in keeping maternal blood glucose within desired levels to prevent complications of maternal hyperglycemia. For this reason, patients are closely monitored for changes in blood glucose after ACS administration.[8]
The conventional ACS regimes: Betamethasone 12 mg IM q24h x 2 doses or dexamethasone 6 mg IM q12h x 4 doses can be used in diabetes. The increased risk of GDM receiving long-term glucocorticoid therapy is well-known. [9,10] The effect of a few doses of corticosteroids on glucose metabolism is less documented, especially in a cohort of persons already at high risk of glucose intolerance. In general, the glycemic effect of steroids begins about 12 hours after the first dose and lasts up to 5 days.[11]
The ideal frequency of monitoring in antenatal women with diabetes is a 7-point profile, including three pre-meal estimations, three post-meal estimations and a 3 am value. This is concordant with recommendations for routine management of GDM.[5]
Previous studies have demonstrated time-dependent changes of maternal hyperglycemia and insulin requirement during ACS therapy in women with gestational diabetes.[12] The time-dependent changes were due to the corticosteroid’s duration of action. Three subsets of patients were observed. The first subset continued to have glucose control with diet alone, the second subset required insulin during the time dependent maternal glycemic changes brought by ACS therapy, and a third subset will require insulin beyond the time dependent maternal glycemic changes.
A few studies looked into the association between ACS administration and GDM mothers. An observational study done by Kakoulidis, et al, at Elena Venizelou General and Maternity Hospital, Athens, Greece on pregnant women with GDM given antenatal steroid therapy noticed a significant need for insulin treatment within the group of women on medical nutrition therapy (MNT) and an increase in insulin dose of 61.4%.[13] It was closely related to steroid dosage, maternal age, and gestational age. In a study by Ramirez-Torres, patients with GDM who were treated by diet alone required insulin de novo in 40% of cases, while those already on insulin needed an increase of 39% to 112% in daily insulin dose.[14] The greatest changes occurred on the second, third and fourth day after ACS therapy. This finding highlights the need for regular glycemic monitoring during this period and a proactive increase in insulin doses, if clinically indicated. However, it failed to present any relationship between maternal characteristics and glycemic changes. Data on these studies were done among Caucasians with different genotype and phenotypic characteristics from Asians.
Medical nutrition therapy should be reinforced in all patients receiving ACS, irrespective of prior glycemic status. High calorie foods should be avoided for up to five days after ACS administration.
Insulin therapy may be required for a short period, after ACS therapy, in women who were previously well controlled on medical nutrition therapy. In patients already on insulin, an increase in dosage or a change in insulin regime may be necessary. If glycemic control is not achieved by increasing the dose of insulin by 20%-30%, it may be advisable to increase the number of injections per day. This can be done by adding rapid-acting insulin by substituting pre-mixed insulin with rapid-acting insulin or by changing basal insulin to pre-mixed or basal bolus regime. In rare cases, intravenous insulin may be needed to achieve glycemic control.[15]
Indications for intravenous insulin include ketoacidosis, highly uncontrolled glycemia not responding to subcutaneous insulin, and fetal or maternal distress deemed due to hyperglycemia.
There is paucity of local data on the factors associated with ACS use and maternal glucose status.
Given this information, this study was conceived to identify and analyze the factors associated with consequent insulin usage after ACS administration in GDM patients. It will help determine the population who would benefit with proactive insulin therapy.
Objectives
To determine the effects of ACS treatment on the glycemia of Filipino women with GDM; to analyze the factors associated with insulin use or increase insulin requirements after ACS administration among GDM patients and to compare the demographic, clinical features, glycemic monitoring and management between GDM mothers on medical nutrition therapy (diet alone) versus medical nutrition therapy and insulin (diet + insulin) prior to ACS administration.
Research Design
This is a retrospective, analytical study. The diagnosis of GDM was based on American diabetes Association (ADA). [16]
Study Population
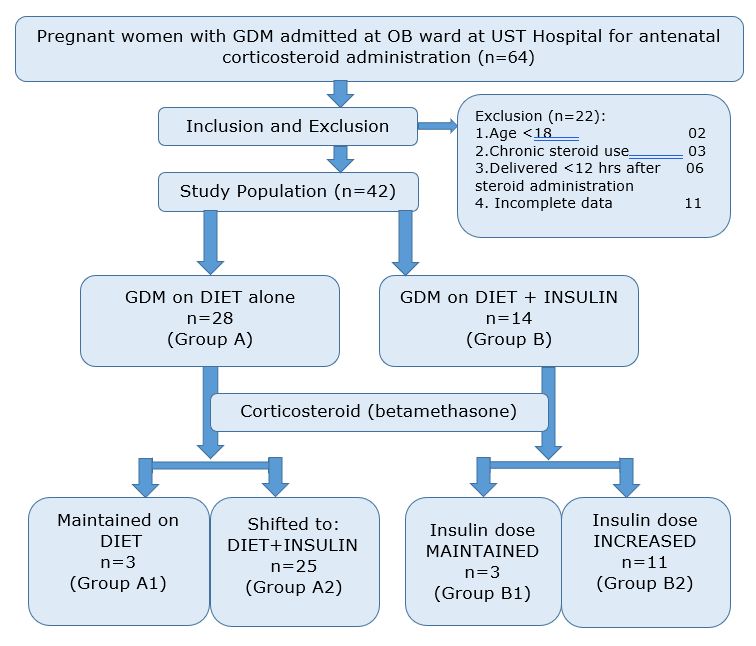
The study included 64 pregnant women with GDM given ACS therapy. All were admitted at the University of Santo Tomas Hospital from January 2017 to December 2019. An indication for ACS administration was decided by the attending obstetrician.
The inclusion criteria was pregnant women who fulfilled the following criteria: admitted at University of Santo Tomas Hospital; 18 years old and above; diagnosed case of GDM and who had ACS drug between 24 to 36 weeks age of gestation for pregnancies at risk for pre-term delivery. Excluded were pregnant women with chronic exposure to steroid therapy for treatment of other maternal conditions (bronchial asthma, allergies, idiopathic thrombocytopenic purpura (ITP) or other autoimmune conditions); termination of pregnancy within 12 hours after ACS administration; and incomplete data for review.
Methodology
This is a retrospective analytical study of pregnant women diagnosed with GDM, admitted at UST Hospital and who received ACS treatment (betamethasone) between 24-36 weeks AOG for fetal lung maturity. ACS was primarily given for pregnancies at risk for premature delivery at the discretion of the attending obstetrician. GDM was diagnosed using 75-g oral glucose tolerance test.
Data were retrieved by review of medical charts and records at USTH from January 2017 to December 2019. There were 64 GDM patients admitted for ACS. Twenty-two subjects were excluded (2 were below 18 years of age, 3 had chronic steroid use, 6 delivered less than 12 hours after administration of ACS and 11 had incomplete data for review). Thus, only 42 patients were included for analysis.
The study population was categorized into two groups in reference to GDM management before the administration of ACS: GDM on diet alone (Group A) and (Group B), requiring insulin treatment. Data recorded included: maternal age, gestational age, family history of DM, diagnosis of GDM on previous pregnancy, indication for steroids, steroid use, and dose, tocolysis, laboratory values used in the diagnosis of GDM (FBS, first and second hour 75-g oral glucose tolerance test (OGTT) and fasting capillary glucose (FCG) and one-hour post-prandial capillary glucose (PPCG) levels. Doses of insulin if given were recorded. Data collection began the day before steroids were given and continued until discharge or delivery.
All women received dietary treatment with or without insulin therapy to achieve a goal of fasting glucose <95 mg/dL and 1-hour post-prandial glucose of <140 mg/dL. Capillary blood glucose levels were monitored every 4 to 6 hours during their hospital stay. The mean duration of observation was five days.
Statistical Method
Data were analyzed using statistical software. Descriptive statistics included mean, standard deviation, frequency and percentage. In order to check for the association between factors and outcomes we performed univariate analysis on each factor. Continuous variables were changed to categorical. The frequencies between groups were compared and statistical significance tested using Fisher’s Exact. A p-value ≤0.05 was considered statistically significant. As the observations were too few, a multivariate analysis was foregone.
Results
Forty-two patients met the study criteria: upon enrollment, 28 were initially controlled on DIET alone (Group A) and 14 were already on insulin (Group B). Among Group A participants, 25/28 required insulin for glucose control (Group A2) after steroid administration. Under Group B, 11/14 required increase in insulin dose after steroid administration (Group B2). Indications leading to admission and steroid administration represent relatively common complications of pregnancy (Table 1).
Table 1. Indication for corticosteroid administration to promote fetal lung maturity.
|
|
Number (n=42) |
Percentage |
|
Preterm Labor |
24 |
57% |
|
Pre-Eclampsia |
10 |
24% |
|
PPROM |
5 |
12% |
|
Placental Abruption |
2 |
5% |
|
Oligohydramnios |
1 |
2% |
The mean age of presentation was 32 years old (±6) (Table 2). About a half of the population had a first degree relative diagnosed with diabetes mellitus (46% and 64% in Group A and Group B, respectively). Frequency of completed steroid dose of 24 mg betamethasone was comparable to both groups (82% and 86%). FBS and first- hour 75-g OGTT was elevated in a greater percentage in Group B while second hour 75-g OGTT was comparable to both groups (Table 3).
Table 2. Demographic profiles of patients with GDM admitted for antenatal corticosteroid administration grouped according to method of glycemic management upon enrollment (n=42).
|
|
DIET (Group A) n = 28 |
DIET + INSULIN (Group B) n = 14 |
|
Age (years) |
32 ± 6 |
32 ± 6 |
|
Obstetrical History |
|
|
|
Primigravida |
4 (14) |
3 (21) |
|
History of Stillbirth |
4 (14) |
5 (36) |
|
History of Preterm Delivery |
5 (18) |
4 (29) |
|
Gestational HTN |
5 (18) |
3 (21) |
|
Family History of DM |
13 (46) |
9 (64) |
|
Past Medical History of GDM |
6 (21) |
8 (57) |
Table 3. FBS and 75-gm OGTT values used in diagnosis of GDM taken at 24-28 weeks AOG (n=42)
|
|
DIET (Group A) n = 28 |
DIET+INSULIN (Group B) n = 14 |
|
FBS (mg/dL) |
89.46 ± 9.54 |
97.54 ± 11.47 |
|
Elevated FBS (≥92 mg/dL) |
12 (43) |
10 (71) |
|
75 g OGTT First Hour (mg/dL) |
171.39 ± 16.48 |
186.90 ± 18.82 |
|
Elevated First Hour (≥180 mg/dL) |
8 (29) |
8 (57) |
|
75 g OGTT Second Hour (mg/dL) |
161.07 ± 16.15 |
158.86 ± 26.29 |
|
Elevated Second Hour (≥153 mg/dL) |
22 (79) |
10 (71) |
|
Frequency of Abnormal OGTT result |
|
|
|
0 |
06 (21) |
02 (14) |
|
1 |
14 (50) |
06 (43) |
|
2 |
08 (29) |
06 (43) |
Figure 1 displays the percentage of population with abnormal fasting and 1-hour post capillary glucose after steroid administration. An elevated FCG was ≥95 mg/dL and elevated one-hour PPCG was ≥140 mg/dL. The day the first dose of corticosteroid was administered was designated as day 1 (D1). Steroids were given on D1 and D2. FCG and one-hour PPCG were both elevated within 24 hours after administration of corticosteroid (betamethasone) in 60%-70% of the population. On day 2-3, the FCG values remained elevated in about 70%. Thereafter, there was a steady decrease to about 30%. The one-hour PPCG was elevated in 85% on day 2 and remained elevated in 70% of women on day 3-4 and reached 53% on day 5. It also showed that FCG tends to return to normal values faster that PPCG after administration of betamethasone.

Figure 1. Percentage with elevated FCG and at least one abnormal one-hour PPCG
Table 4 presents the population who were controlled on DIET alone upon enrollment (Group A) and subcategorized into two groups according to the method of glycemic management after administration of ACS: 1) GDM women who remained euglycemic with diet alone (Group A1) and 2) GDM women on diet previously but now required insulin treatment for euglycemia (Group A2). Comparison of their profile was done and statistical significance was determined using the Fisher’s exact test. A p-value of <0.05 was conclusive to be statistically significant.
Among the maternal factors associated, it was only the AOG upon ACS administration that reached statistical significance. GDM women who were given steroid at 31 weeks AOG or later were associated with subsequent need for insulin treatment (p = 0.03) for glycemic control. In terms of maternal outcome, those who had good glucose control and maintained on diet alone were more likely to deliver through normal spontaneous delivery (NSD) (67%). However, it was not statistically significant.
Table 4. Association of factors among GDM on diet (Group A) on antenatal corticosteroid therapy in insulin initiation (n = 28).
|
DIET (GroupA1) n = 3 |
DIET + INSULIN (GroupA2) n = 25 |
p-value |
|
|
Age groups |
|
|
|
|
<25 |
0 (0) |
2 (8) |
1.0 |
|
25 – 29 |
1 (33) |
7 (28) |
|
|
30 – 34 |
1 (33) |
5 (20) |
|
|
≥35 |
1 (33) |
11 (44) |
|
|
Obstetrical History |
|
|
|
|
Primigravida |
- |
4 (16) |
1.0 |
|
History of Stillbirth |
- |
4 (16) |
1.0 |
|
History of Preterm Delivery |
1 (33) |
4 (16) |
0.46 |
|
History of Gestational HTN |
1 (33) |
4 (16) |
0.46 |
|
Elevated FBS |
2 (67) |
10 (40) |
0.56 |
|
Elevated OGTT First Hour |
1 (33) |
7 (28) |
1.0 |
|
Elevated OGTT Second Hour |
2 (67) |
20 (80) |
0.53 |
| Frequency of Abnormal OGTT Result |
|
|
|
|
1 |
1 (33) |
13 (52) |
0.78 |
|
2 |
1 (33) |
7 (28) |
|
|
Completed Steroid Dose |
2 (67) |
21 (84) |
0.46 |
| AOG at Steroid Administration |
|
|
|
|
27 – 28 |
- |
- |
0.03 |
|
30 – 31 |
1 (33) |
- |
|
|
31 – 32 |
2 (67) |
6 (24) |
|
|
32 – 33 |
- |
6 (24) |
|
|
33 – 34 |
- |
5 (20) |
|
|
34 – 35 |
- |
8 (32) |
|
|
Mode of Delivery |
|
|
|
|
NSD |
2 (67) |
11 (44) |
0.58 |
|
LTCS |
1 (33) |
14 (56) |
|
Figure 2 demonstrates the insulin requirement needed to maintain glucose control. Average insulin per kg body weight was computed. The day the first dose of corticosteroid was administered was designated as day 1 (D1). Steroids were given on day 1 and day 2. Insulin requirement within 24 hours after steroid was at 0.3 units/kBW. There was a steady increase with maximum requirement observed on day 4 and decreased thereafter to 0.33 units/kBW on day 5.
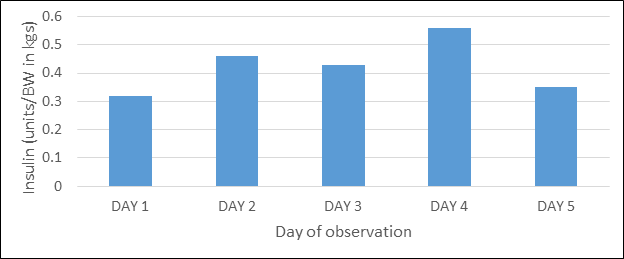
Figure 2. Insulin requirement (dose) in GDM on antenatal corticosteroid therapy (Group A2)
Of the 33% (n=14) of patients enrolled under the DIET + INSULIN (Group B) insulin dose was maintained in only 3 (Group B) patients and insulin was increased further in 11 (Group B2) patients (Table 5). Results showed that none of the maternal risk factors have significant association with increased insulin requirement after administration of steroid. An increase in insulin requirement was seen in all GDM women with a history of stillbirth and preterm delivery. Primigravid GDM women were more likely to be maintained on their insulin requirement even after steroid administration. However, both did not reach statistical significance.
Table 5. Association of factors among GDM with insulin (Group B) on antenatal corticosteroid administration in increased insulin requirement (n=14).
|
|
Insulin Maintained (Group B1)
n = 3 |
Insulin Increased (Group B2) n = 11 |
p-value |
|
Age groups |
|
|
|
|
< 25 |
- |
2 (18) |
0.10 |
|
25 – 29 |
2 (67) |
- |
|
|
30 – 34 |
- |
3 (27) |
|
|
≥ 35 |
1 (33) |
6 (55) |
|
|
Obstetrical History |
|
|
|
| Primigravida |
2 (67) |
1 (33) |
0.93 |
| History of Stillbirth |
- |
5 (45) |
0.26 |
| History of Preterm Delivery |
- |
4 (36) |
0.50 |
| History of Gestational HTN |
1 (33) |
2 (18) |
1.0 |
|
Elevated FBS |
3 (100) |
7 (64) |
0.50 |
|
Elevated OGTT First Hour |
1 (33) |
7 (64) |
0.54 |
|
Elevated OGTT Second Hour |
3 (100) |
7 (64) |
0.50 |
| Frequency of Abnormal OGTT |
|
|
|
|
1 |
2 (67) |
4 (36) |
1.0 |
|
2 |
1 (33) |
5 (45) |
|
|
Administration of Tocolysis |
1 (33) |
6 (55) |
1.0 |
|
Complete Steroid Dose |
3 (100) |
9 (82) |
1.0 |
| AOG at Steroid Administration |
|
|
|
|
27 – 28 |
- |
1 (9) |
0.44
|
|
29 – 30 |
- |
2 (18) |
|
|
30 – 31 |
1 (33) |
- |
|
|
31 – 32 |
- |
1 (9) |
|
|
32 – 33 |
- |
4 (36) |
|
|
33 – 34 |
2 (67) |
3 (27) |
|
|
Mode of Delivery |
|
|
|
|
NSD |
2 (67) |
7 (64) |
1.0 |
|
LTCS |
1 (33) |
4 (36) |
|
Increase in insulin pattern from baseline prior to steroid administration is presented in Figure 3. There was a steep rise of insulin requirement from day 1-2 reaching to 140% increase in insulin dose on day 2. Thereafter, there was a gradual decrease of insulin dose almost returning to the original dose at 20% on day 5.
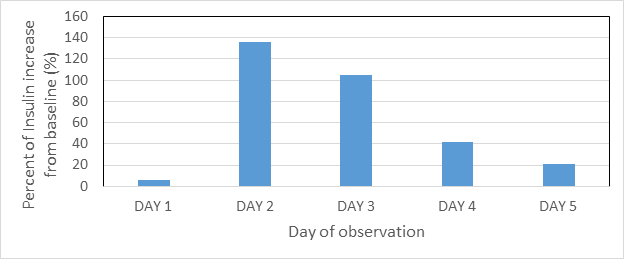
Figure 3. Percent of insulin increase from baseline in GDM on insulin with antenatal corticosteroid (Group B2)
Discussion
Our study demonstrated that hyperglycemia as a side effect of ACS administration was seen in the majority of subjects, regardless if they were initially controlled on medical nutrition therapy alone or with insulin therapy. The duration of hyperglycemia was at 3-5 days post steroid administration.
A proactive approach to insulin dose modification may control hyperglycemia after ACS and avoid deleterious effects to both the mother and fetus. An increase in dose of 16% to 40% has been recommended in two studies. [17,18] In this approach, adjustment is done shortly after glucocorticoid treatment for fetal lung maturation in diabetic women prevents severe dysregulation of metabolic control.
The only factor associated with insulin usage in our study is gestational age at steroid administration on those who were diet controlled upon enrollment. The later the betamethasone was administered in a GDM mother, the higher was her risk to require insulin. This finding is consistent with one of the pathophysiologic mechanisms of GDM. As explained earlier, pregnancy induces a state of insulin resistance. One of its mechanisms of insulin resistance in GDM is the progressive increase in counter-regulatory hormones.[19] The hormones include placental growth hormone (GH), glucocorticoid cortisol, progesterone and inflammatory cytokine TNF. TNF impairs insulin signaling by diminishing insulin receptor tyrosine kinase activity and also suppression of adiponectin, the endogenous insulin-sensitizing hormone. Altinova, et al., supported this hypothesis by investigating levels of adiponectin and TNF and their association with GDM.[20] Therefore, the increase in counter-regulatory hormones as pregnancy progresses in addition to maternal metabolic effects of administered steroid intensifies insulin resistance in GDM. As a consequence, maternal hyperglycemia becomes worse explaining the subsequent need of insulin for blood glucose control.
On the other hand, this association was not seen in Group B (diet + insulin). This may be due to the fact that insulin was already part of the management. The presence of insulin attenuates the increase in maternal hyperglycemia as a result of steroid use in this group.
There have been no other studies to the best of our knowledge that looked into the association of insulin usage, specifically in GDM mothers given ACS therapy (betamethasone) for at-risk premature delivery. Nevertheless, we looked into other studies regarding characteristic maternal risk factors that predict insulin therapy in GDM per se. Bakiner, et al. assessed the association between insulin need in GDM with clinical features and laboratory parameters.[21] They found that the independent predictors for insulin therapy were found as fasting plasma glucose on OGTT levels during diagnosis in GDM. Another study done by Wong, et al., assessed patient factors that predict failure of medical nutritional therapy thus necessitating insulin therapy.[22] On multivariate logistic regression analysis, BMI, fasting glucose level and 2-hour glucose level on OGTT and gestational week when GDM was diagnosed were all independent predictors for requirement of insulin therapy. None of these risk factors were significant with our specific population (GDM on ACS therapy) on this study. However, the lack of association may be due to small sample size.
Pregnancy outcome (mode of delivery) did not show any significant association and was comparable to all groups.
Conclusion
Our study showed that among the maternal factors studied, the timing (>31 weeks AOG) of administration of ACS on GDM mothers is associated with subsequent insulin initiation, but only on patients initially controlled on diet alone. The rise in maternal hyperglycemia was observed in a majority of patients within 24 hours after first ACS dose with a mean duration of 4-5 days.
LIMITATIONS
The major limitation of our study was the small study population which can reduce the power of our study. Another limitation was the retrospective nature which threatens the quality of data collected.
RECOMMENDATION
Based on the limitation of this study, we recommend that a prospective case-controlled study be conducted using a larger population to study the predictors of insulin usage and maternal glucose changes on GDM mothers given ACS therapy.
ETHICAL CONSIDERATIONS
This study used human subjects in accordance with the International Conference on Harmonization (ICH) Guidelines on Good Clinical Practice (GCP). It was subjected to the University of Santo Tomas Hospital Institutional Review Board (USTH-IRB) for approval prior to its commencement.
- Men-Jean Lee DG. Antenatal corticosteroid therapy for reduction of neonatal respiratory morbidity and mortality from preterm delivery. Charles J Lockwood, Richard Martin, Vanessa A Barss, eds. UptoDate Inc. Wolters Kluwer; 2018.
- Saccone G, Berghella V. Antenatal corticosteroids for maturity of term or near term fetuses: systematic review and meta-analysis of randomized controlled trials. BMJ [Internet]. 2016;355:i5044. Available from: http://dx.doi.org/10.1136/bmj.i5044
- Committee on Obstetric Practice. Committee opinion no. 713: Antenatal corticosteroid therapy for fetal maturation. Obstet Gynecol [Internet]. 2017;130(2):e102–9. Available from: http://dx.doi.org/10.1097/AOG.0000000000002237
- Kazem M, Hutcheon JA, Joseph KS. A population-based study of antenatal corticosteroid prophylaxis for preterm birth. J Obstet Gynaecol Can [Internet]. 2012;34(9):842–8. Available from: http://dx.doi.org/10.1016/S1701-2163(16)35383-X
- Metzger BE, Buchanan TA, Coustan DR, de Leiva A, Dunger DB, Hadden DR, et al. Summary and recommendations of the fifth international workshop-conference on gestational diabetes mellitus. Diabetes Care [Internet]. 2007;30 Suppl 2 (Supplement_2):S251-60. Available from: http://dx.doi.org/10.2337/dc07-s225
- Walker JD. NICE guidance on diabetes in pregnancy: management of diabetes and its complications from preconception to the postnatal period. NICE clinical guideline 63. London, March 2008. Diabet Med. 2008 Sep;25(9):1025-7. doi: 10.1111/j.1464-5491.2008.02532.x. PMID: 19183306.
- Kitzmiller JL, Block JM, Brown FM, Catalano PM, Conway DL, Coustan DR, et al. Managing preexisting diabetes for pregnancy: summary of evidence and consensus recommendations for care. Diabetes Care [Internet]. 2008;31(5):1060–79. Available from: http://dx.doi.org/10.2337/dc08-9020
- Schäcke H, Döcke WD, Asadullah K. Mechanisms involved in the side effects of glucocorticoids. Pharmacol Ther [Internet]. 2002;96(1):23–43. Available from: http://dx.doi.org/10.1016/s0163-7258(02)00297-8
- Ha Y, Lee K-H, Jung S, Lee S-W, Lee S-K, Park Y-B. Glucocorticoid-induced diabetes mellitus in patients with systemic lupus erythematosus treated with high-dose glucocorticoid therapy. Lupus [Internet]. 2011;20(10):1027–34. Available from: http://dx.doi.org/10.1177/0961203311402246
- Yildirim Y, Tinar S, Oner RS, Kaya B, Toz E. Gestational diabetes mellitus in patients receiving long-term corticosteroid therapy during pregnancy. J Perinat Med [Internet]. 2006;34(4):280–84. Available from: http://dx.doi.org/10.1515/JPM.2006.053
- Miracle X, Renzo D, Stark GC, Fanaroff A, Carbonell-Estrany A, Saling X. Coordinators of world association of perinatal medicine prematurity working group. Guideline for the use of antenatal corticosteroids for fetal maturation. J Perinat Med. 2008;36:191–6.
- Itoh A, Saisho Y, Miyakoshi K, Fukutake M, Kasuga Y, Ochiai D, et al. Time-dependent changes in insulin requirement for maternal glycemic control during antenatal corticosteroid therapy in women with gestational diabetes: a retrospective study. Endocr J [Internet]. 2016;63(1):101–4. Available from: http://dx.doi.org/10.1507/endocrj.EJ15-0482
- Kakoulidis I, Ilias I, Linardi A, Milionis C, Michou A, Koukkou E. Glycemic profile assessment during betamethasone administration in women with gestational diabetes mellitus. Diabetes Metab Syndr [Internet]. 2019;13(1):214–5. Available from: http://dx.doi.org/10.1016/j.dsx.2018.08.001
- Ramírez-Torres MA, Pérez-Monter SE, Espino y Sosa S, Ibargüengoitia-Ochoa F. Effect of betamethasone in blood glucose levels in pregnant diabetic women at risk of preterm birth. Ginecol Obstet Mex. 2011;79(9):565–71.
- Kalra S, Kalra B, Gupta Y. Glycemic management after antenatal corticosteroid therapy. N Am J Med Sci [Internet]. 2014;6(2):71–6. Available from: http://dx.doi.org/10.4103/1947-2714.127744
- Standards of medical care in diabetes. Diabetes Care. 2018;41:S7–12.
- Kreiner A, Gil K, Lavin J. The effect of antenatal corticosteroids on maternal serum glucose in women with diabetes. Open J Obstet Gynecol [Internet]. 2012;02(02):112–5. Available from: http://dx.doi.org/10.4236/ojog.2012.22021
- Mathiesen ER, Christensen A-BL, Hellmuth E, Hornnes P, Stage E, Damm P. Insulin dose during glucocorticoid treatment for fetal lung maturation in diabetic pregnancy: test of an algorithm [correction of analgorithm]. Acta Obstet Gynecol Scand [Internet]. 2002;81(9):835–9. Available from: http://dx.doi.org/10.1034/j.1600-0412.2002.810906.x
- Barbour LA, McCurdy CE, Hernandez TL, Kirwan JP, Catalano PM, Friedman JE. Cellular mechanisms for insulin resistance in normal pregnancy and gestational diabetes. Diabetes Care [Internet]. 2007;30 Suppl 2 (Supplement_2):S112-9. Available from: http://dx.doi.org/10.2337/dc07-s202 .
- Altinova AE, Toruner F, Bozkurt N, Bukan N, Karakoc A, Yetkin I, et al. Circulating concentrations of adiponectin and tumor necrosis factor-alpha in gestational diabetes mellitus. Gynecol Endocrinol [Internet]. 2007;23(3):161–5. Available from: http://dx.doi.org/10.1080/09513590701227960 .
- Bakiner O, Bozkirli E, Ozsahin K, Sariturk C, Ertorer E. Risk factors that can predict antenatal insulin need in gestational diabetes. J Clin Med Res [Internet]. 2013;5(5):381–8. Available from: http://dx.doi.org/10.4021/jocmr1515w
- Wong VW, Jalaludin B. Gestational diabetes mellitus: who requires insulin therapy?: GDM: who requires insulin therapy? Aust N Z J Obstet Gynaecol [Internet]. 2011;51(5):432–6. Available from: http://dx.doi.org/10.1111/j.1479-828X.2011.01329.x
![]() Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0
International License, which permits use, share — copy and redistribute the material in any medium or format,
adapt — remix, transform, and build upon the material, as long as you give appropriate credit,
provide a link to the license, and indicate if changes were made. You may do so in any reasonable manner,
but not in any way that suggests the licensor endorses you or your use. You may not use the material for
commercial purposes. If you remix, transform, or build upon the material, you must distribute your
contributions under the same license as the original. You may not apply legal terms or technological
measures that legally restrict others from doing anything the license permits. The images or other
third party material in this article are included in the article’s Creative Commons license, unless indicated
otherwise in a credit line to the material. If material is not included in the article’s Creative Commons
license and your intended use is not permitted by statutory regulation or exceeds the permitted use,
you will need to obtain permission directly from the copyright holder. To view a copy of this license,
visit https://creativecommons.org/licenses/by-nc-sa/4.0/.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0
International License, which permits use, share — copy and redistribute the material in any medium or format,
adapt — remix, transform, and build upon the material, as long as you give appropriate credit,
provide a link to the license, and indicate if changes were made. You may do so in any reasonable manner,
but not in any way that suggests the licensor endorses you or your use. You may not use the material for
commercial purposes. If you remix, transform, or build upon the material, you must distribute your
contributions under the same license as the original. You may not apply legal terms or technological
measures that legally restrict others from doing anything the license permits. The images or other
third party material in this article are included in the article’s Creative Commons license, unless indicated
otherwise in a credit line to the material. If material is not included in the article’s Creative Commons
license and your intended use is not permitted by statutory regulation or exceeds the permitted use,
you will need to obtain permission directly from the copyright holder. To view a copy of this license,
visit https://creativecommons.org/licenses/by-nc-sa/4.0/.