Effect of Selenium Supplementation on Mild Graves’ Ophthalmopathy at a Tertiary Hospital – a Six-Month, Open-Labelled, Assessor-Masked, Randomized Controlled Trial
Joy Mangubat Flores, Niña Angelica G. Sioson, Armida L. Suller-Pansacola, Jean D. Uy-Ho
Apr 2025 DOI 10.35460/2546-1621.2025-0002

Introduction
Graves’ ophthalmopathy (GO) is an autoimmune inflammation of the orbital tissues closely associated with autoimmune thyroid diseases.[1,2] Also referred to as Graves’ orbitopathy, Graves’ eye disease, thyroid eye disease and thyroid-associated ophthalmopathy, GO is the most prevalent orbital disorder and most common cause of unilateral and bilateral proptosis in adults.[1-4] It is the most common extrathyroidal manifestation of Graves’ disease affecting 25%-50% of patients.[1,2,5] It typically develops concurrently with hyperthyroidism but may also precede or follow its onset.2 Although uncommon, it can occur in patients with euthyroid or hypothyroid chronic autoimmune thyroiditis.[6]
The disease is more prevalent in female patients than in their male counterparts, with an annual incidence of 16 per 100,000 in women and 3 per 100,000 in men.[2] Among Asians, the prevalence of GO associated with hyperthyroidism ranges from 35% to 60%.[3] In the Philippines, a study by Palisoc, et al., (2010) reported a prevalence of 48%, with the condition occurring more frequently in patients aged between 30 and 49 years. The most common symptom identified was eye pain; while the predominant signs included eyelid retraction, proptosis and lid lag.[7] The natural history of GO features an initial active phase characterized by alternating acute inflammatory episodes and remissions, followed by stabilization (plateau phase) and ends with an inactive or burn-out phase, which typically involves regression over a period of 12 to 18 months.[6,8]
Diagnosed clinically based on symptoms and ocular signs, mild GO is frequently misdiagnosed as conjunctivitis or allergic reactions, resulting in delays in both diagnosis and treatment, which can exacerbate the condition.[2,9] Therefore, a thorough clinical examination is essential for accurate diagnosis; in cases of uncertainty, the opinion of an ophthalmologist is important.[8] Spontaneous remission is often observed in minimal-to-mild GO; however, complete resolution is rare when the condition is more than mild.[6] Early diagnosis, management of modifiable risk factors and prompt treatment of mild forms of GO can effectively limit the risk of progression to more severe forms. At this time, more severe forms of GO present a therapeutic challenge, often necessitating prolonged and multiple medical and surgical interventions, which can significantly impact the quality of life of affected individuals.[6] Previously, a wait-and-see approach was adopted for patients with mild GO, as spontaneous improvement was anticipated, requiring only local measures such as artificial tears and ointments to manage symptoms.
Graves’ orbitopathy is associated with increased oxidative stress. Selenium, known for its antioxidant and immunoregulatory properties, has been proposed as an adjuvant therapy for patients with mild GO.[6] In a randomized, double-blind, placebo-controlled trial conducted in Europe in 2011, Marcocci, et al., identified that selenium administration significantly improved quality of life, reduced ocular involvement and slowed disease progression patients with mild GO.[10] Consequently, six-month selenium supplementation for patients diagnosed with mild GO was included as a recommendation in the 2016 European Thyroid Association/European Group on Graves’ Orbitopathy Guidelines for the Management of Graves’ Orbitopathy.[4] However, this recommendation is not endorsed by the American Thyroid Association, as patients in the United States are usually not selenium deficient and thus not in need of supplementation.[10]
To our knowledge and from our review of literature, there is a paucity of prior local studies investigating the effects of selenium supplementation on mild GO in Filipino patients. This study aimed to compare the efficacy of standard care (eye drops) with that of standard care combined with selenium supplementation. The objective was to determine whether selenium supplementation over a six-month period could reduce clinical signs and prevent progression of mild GO. Specific objectives included comparing baseline and six-month assessments of visual acuity, color vision and soft tissue signs between the selenium and control groups, as well as evaluating the percentage change in these parameters and the CAS over the study period.
Methodology
Research Design
An open-labelled, assessor-masked, randomized controlled trial was conducted on adult patients diagnosed with mild GO. Patients were given 200 mcg of selenium daily in addition to standard care or standard of care alone, over a six-month period. The study commenced following approval from the University of Santo Tomas Hospital Research Ethics Committee (USTH REC). It adhered to both national and international ethical guidelines such as the International Council for Harmonisation Good Clinical Practice (ICH-GCP), National Ethical Guidelines for Health and Health-Related Research (NEGHHRR) 2017 and the Data Privacy Act of 2012, along with its Implementing Rules and Regulations of 2016.
Study Population
This study included patients aged 18 to 60 years with a history of Graves’ hyperthyroidism who presented at least one sign of mild GO. The qualifying signs included minor lid retraction of less than 2 mm, mild soft tissue involvement, exophthalmos measuring less than 3 mm above normal and corneal exposure responsive to lubricants. Additionally, participants had to have disease duration of less than 18 months.
The exclusion criteria enlist a range of conditions that could confound the study results. Specifically, patients with soft tissue swelling classified as NO SPECS class 2c (eg, severe chemosis or severe eyelid swelling) were excluded, as were those with proptosis exceeding 19.5 mm. Other exclusions are the presence of diplopia in the primary or reading position, ocular torticollis and any restriction in mono-ocular duction of less than 20 degrees in any direction. Patients exhibiting signs or symptoms of optic nerve involvement, those with a history of ophthalmopathy treatment beyond local measures (eg, eye drops) and individuals with a history of drug and/or alcohol abuse were also excluded. In addition, patients with severe concomitant illnesses and pregnant individuals were not eligible for participation; any patient who became pregnant during the course of the study was similarly excluded.
Sample Size
Sample size computation for analysis of covariance (ANCOVA) was conducted using GPower version 3.1.9.7. The researchers used parameters estimated by Marcocci, et al. (2011), taking into account the change at six-month appearance GO-QOL score among patients with selenium (10.6 +/- 10.9) versus patients treated with standard care (-2.6 +/- 11.7).[10] With a power of 95% at a significance level of 5% (two-tailed), a minimum sample size of 42 respondents was necessary. Considering the study design, the total sample size was divided into two groups, thus each group had 21 respondents.
Outcome Measurements
The primary outcome was the objective assessment of ocular changes conducted by masked ophthalmologists. The secondary outcome was measured using the clinical activity score (CAS), in accordance with the European Group on Graves’ Orbitopathy (EUGOGO) recommendations for assessing response to interventions in clinical trials. Data were collected at baseline, third month of treatment and sixth month.
A beneficial response was defined as improvement in at least one eye without any deterioration in both eyes, based on the following criteria: an increase in lid aperture of ≥2 mm; improvement by at least one grade in eyelid swelling, eyelid erythema, conjunctival redness or conjunctival edema; improvement in best-corrected visual acuity (BCVA) by ≥2 lines on the Bailey-Lovie chart, or substantial improvement in color vision.
Deterioration was defined as an increase in lid aperture of ≥2 mm; worsening by at least one grade in eyelid swelling, eyelid erythema, conjunctival redness or conjunctival edema; an increase in exophthalmos of ≥2 mm; the appearance of diplopia or limitation of eye movement; or decline in BCVA by ≥2 lines, substantial changes in color vision, visual fields, optic disc appearance or development of a relative afferent pupillary defect.
Study Procedure and Data Collection
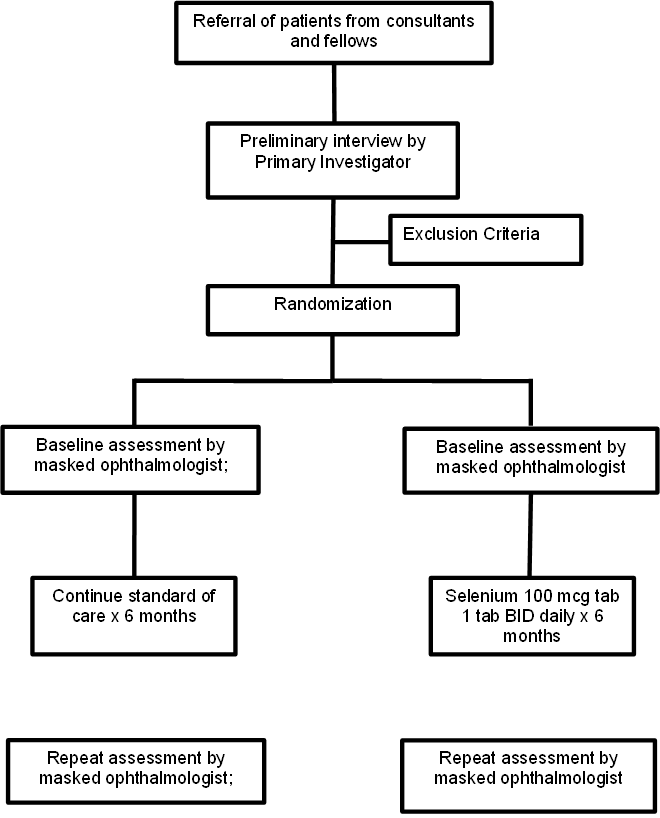
Figure 1. Flowchart for methodology
Recruitment Process and Informed Consent
Study recruitment was initiated with the investigators obtaining patient referral from consultants and fellows of the Section of Endocrinology, Diabetes and Metabolism of the UST hospital. Referrals were sourced from private clinics or the hospital’s Ambulatory Care Services Department. During the pandemic, patient recruitment also took place through the teleconsultation platform of the UST Hospital Endocrinology Ambulatory Care Services. Patients underwent a preliminary screening interview following the inclusion exclusion criteria, conducted by the primary investigator to ensure eligibility.
To participate, patients received a detailed explanation of the purpose of study as well as the study procedure, schedule of follow-up, duration of treatment, benefits and any possibility of adverse event/s or withdrawal from the study. They were then asked to sign the written informed consent following previously mentioned ethical guidelines. Researchers who are members of the healthcare team of recruited patients were not involved in obtaining informed consent for those specific patients.
Randomization and Monitoring
Once patients were confirmed eligible and have consented to the study, they were randomized to one of two groups: the treatment arm (selenium 100 mcg/capsule, one capsule taken orally twice daily for six months) or the standard of care arm (no selenium, only standard of care). Randomization was performed using sealed envelopes, whereby, after providing consent, a patient was assigned a treatment regimen based on the contents of the envelope. Patients were aware of their treatment allocation (open-label), but the ophthalmologists performing assessments were masked to the treatment group.
Ophthalmologic assessments were conducted at three time points: baseline, three months after treatment initiation and six months after observation concluded. The three-month assessments aimed at evaluating any improvements or worsening of GO based on the assigned treatment arm.
The ophthalmologic assessments included several processes: visual acuity testing, external eye examination, extraocular movements’ assessment, intraocular pressure measurement, margin-to-reflex distance measurement, optic nerve visualization, tear up break time evaluation, fluorescein dye testing and exophthalmometry. These examinations were performed at no cost to participants at the Ophthalmology Clinic of the UST Hospital Ambulatory Care Services.
To objectively assess ophthalmologic changes, the EUGOGO Case Record Form was used covering the following parameters: lid aperture, soft tissue involvement, proptosis, eye muscle involvement and visual acuity using Baily-Lovie chart. The CAS, which consists of seven items (spontaneous retrobulbar pain, pain during attempted up- or down-gaze, conjunctival redness, eyelid redness, chemosis, swelling of the caruncle and eyelid swelling) was recorded during the three time points as well. The score is the sum of aforementioned items.
Safety and Tolerability Assessment
Selenium is known to be readily absorbed and has not been associated with significant side effects. Throughout the study, any subjective complaints from patients were recorded similarly during the three time points. This was done to ensure safety and tolerability. All complaints or adverse events were documented as part of routine safety assessment during the course of the trial, ensuring that any potential adverse events were appropriately managed.
Withdrawal Criteria
The analysis was conducted using the “intention-to-treat” approach. For instance, patients who withdrew from the study due to non-compliance or worsening of their eye condition, which required specific eye treatment, were included in the primary analysis. The results from the last recorded visit were carried forward and evaluated as the final visit. Only patients who were lost to follow-up before the second visit at the three-month mark were excluded from the analysis.
Confounders
Potential confounders to this study include intake of multivitamins, as well as other antioxidants like glutathione by patients. This was noted upon enrolment of patients to the study.
Statistical Analysis
Descriptive statistics was used to summarize the demographic and clinical characteristics of patients. Frequency and proportion were used for categorical variables, median and interquartile range for non-normally distributed continuous variables, and mean and standard deviation for normally distributed continuous variables. Independent sample t-test, Mann-Whitney U test and Fisher’s Exact/Chi-square test was used to determine the difference of mean, rank and frequency, respectively, between patients with selenium versus patients treated with standard of care. Paired sample t-test, Wilcoxon signed-rank test and McNemar test was used to determine the difference of mean, rank and frequency, respectively, on patients from initial to third month or sixth month observation. All statistical tests were two-tailed tests. Shapiro-Wilk test was used to test the normality of continuous variables. Missing values were neither replaced nor estimated. Null hypotheses were rejected at 0.05α-level of significance. STATA 13.1 was used for data analysis.
Ethical Considerations
Privacy and Confidentiality
The study ensured privacy and confidentiality of patient records by storing collected data in a password-protected electronic database, which may contain personal identifiers. A de-identified version of database was provided to the statistician and other authorized personnel. All paper-based data were securely stored in a locked cabinet. Access to collected data and research-related documents was restricted to members of the research team. However, if necessary, access may be granted to the USTH REC for verification purposes only. All collected data will be retained for a maximum of three years and destroyed thereafter by shredding, while electronic data will be disposed of by reformatting the electronic hard drive.
Benefits
Patients did not receive any reimbursement, compensation or incentives from this study. However, information from the study will help the population affected with mild GO as this can further strengthen/weaken the 2016 EUGOGO recommendation of six-month selenium supplementation and its implementation among Filipino patients.
Risks and Inconvenience
Selenium when taken below the daily intake limit of 400 mcg is generally not associated with side effects. However, one study, titled “Selenium Supplementation and Secondary Prevention of Nonmelanoma Skin Cancer” by Duffield-Lillico, et al., (JNCI: Journal of the National Cancer Institute, Volume 95, Issue 19, 1 October 2003, Pages 1477–1481) reported that “individuals at high risk of non-melanoma skin cancer continue to demonstrate that selenium supplementation increases the risk of squamous cell carcinoma and total non-melanoma skin cancer.”[11] To date, this is the only published risk of selenium supplementation.
Any expenses related to side effects or adverse reactions/events occurring during this clinical trial were shouldered by the investigators.
Results
A total of 42 participants were included in the study, half of which was randomized to the selenium group and half assigned to the standard of care group. Both arms were composed of predominantly female sex with median duration of ophthalmologic symptoms of five months for the selenium group and four months for the standard of care group. There were no reports of side effects or adverse events noted.
Table 1. Baseline Characteristics of Study Population
| Characteristic |
Selenium (n=21) |
Standard of Care (n=21) |
| Age - yrs |
31 ± 10 |
32 ± 7 |
| Female sex – number of patients (%) |
19 (90.4) |
17 (80.9) |
| Duration of ophthalmologic symptoms - months |
5 |
4 |
Table 2 presents the findings of eye examinations conducted over three time points, which included the key parameters of best VA (BVA), relative afferent pupillary defect (RAPD) and color vision. At the initial assessment, there were no significant differences between the two groups as to BVA and color vision. There were no instances of RAPD in either group. At the three-month assessment, follow-up indicated a significantly higher BVA for the selenium group (median of 0.1, IQR 0 to 0.2 vs 0, IQR 0 to 0.1; p = 0.030) compared to the standard of care group. Additionally, the color vision demonstrated significant difference between groups, with the selenium group having a mean score of 14.9 (SD 0.37) compared to standard of care group (14.62, SD 0.73, p = 0.027). By the six-month follow-up, there was no significant difference in BVA and color vision between the two groups. Comparative analysis between initial and subsequent assessments also revealed no significant changes for either treatment group at both follow-ups.
Table 2. Eye Examination Findings at Three Time Points
|
Treatment group |
P-value |
|||
|
Total (n=84) |
Selenium (n=42) |
Standard of Care (n=42) |
||
|
Frequency (%); Mean ± SD; Median (IQR) |
||||
|
Initial |
|
|
|
|
| BVA |
0 (0 to 0.2) |
0.1 (0 to 0.2) |
0 (0 to 0.2) |
0.389 |
| RAPD |
0 |
0 |
0 |
- |
| Color Vision |
14.75 ± 0.60 |
14.74 ± 0.54 |
14.76 ± 0.66 |
0.857 |
|
3 rd month |
|
|
|
|
| BVA |
0 (0 to 0.2) |
0.1 (0 to 0.2) |
0 (0 to 0.1) |
0.030 |
| RAPD |
0 |
0 |
0 |
- |
| Color Vision |
14.76 ± 0.59 |
14.90 ± 0.37 |
14.62 ± 0.73 |
0.027 |
|
6 th month |
|
|
|
|
| BVA |
0 (0 to 0.2) |
0.1 (0 to 0.2) |
0 (0 to 0.2) |
0.126 |
| RAPD |
0 |
0 |
0 |
- |
| Color Vision |
14.69 ± 0.64 |
14.76 ± 0.53 |
14.62 ± 0.73 |
0.309 |
|
Initial vs 3 rd month |
|
|
|
|
| BVA |
0.420 |
0.951 |
0.197 |
|
| RAPD |
- |
- |
- |
|
| Color Vision |
0.897 |
0.104 |
0.349 |
|
|
Initial vs 6 th month |
|
|
|
|
| BVA |
0.269 |
0.652 |
0.242 |
|
| RAPD |
- |
- |
- |
|
| Color Vision |
0.534 |
0.840 |
0.349 |
|
Eyelid position findings, which included palebral aperture, upper lid retraction, lower lid retraction, lagophthalmos and lateral flare are noted in Table 3. At the initial and three-month assessment, there were no significant differences between the two groups across the measured parameters. By the six-month follow-up, significant differences emerged in lower lid retraction, where a median of 1 m (IQR: 0 to 1, p = 0.009) was recorded for both groups. Comparing the initial and six-month assessments, a significant change was noted for lower lid retraction for the selenium group (p = 0.002). For the other time points, there was insufficient evidence to state a statistically significant difference.
Table 3. Eyelid Position Findings
|
Treatment group |
P-value |
|||
|
Total (n=84) |
Selenium (n=42) |
Standard of Care (n=42) |
||
|
Frequency (%); Median (IQR) |
||||
|
Initial |
|
|
|
|
| 1st Fixation |
0 |
0 |
0 |
- |
| Palpebral Aperture, mm |
9 (8 to 11) |
9 (8 to 11) |
9 (8 to 11) |
0.480 |
| Upper Lid Retract, mm |
0 (0 to 1) |
0 (0 to 0) |
0 (0 to 1) |
0.648 |
| Lower Lid Retract, mm |
1 (0 to 1) |
1 (0 to 1) |
1 (0 to 1) |
0.543 |
| Lagopthalmos |
0 (0 to 1) |
0 (0 to 1) |
0 (0 to 1) |
0.409 |
| Lateral Flare |
0 |
0 |
0 |
- |
|
3 rd month |
|
|
|
|
| 1st Fixation |
0 |
0 |
0 |
- |
| Palpebral Aperture, mm |
9 (8 to 10) |
9 (8 to 10) |
9 (8 to 10) |
0.756 |
| Upper Lid Retract, mm |
0 (0 to 0) |
0 (0 to 0) |
0 (0 to 0) |
0.273 |
| Lower Lid Retract, mm |
1 (0 to 1) |
1 (0 to 1) |
1 (0 to 1) |
0.808 |
| Lagopthalmos |
0 (0 to 1) |
0 (0 to 1) |
0 (0 to 1) |
0.885 |
| Lateral Flare |
3 (3.57) |
3 (7.14) |
0 |
0.241 |
|
6 th month |
|
|
|
|
| 1st Fixation |
0 |
0 |
0 |
- |
| Palpebral Aperture, mm |
9 (8 to 10) |
9 (8 to 9) |
9 (8 to 10) |
0.815 |
| Upper Lid Retract, mm |
0 (0 to 0) |
0 (0 to 0) |
0 (0 to 0) |
0.100 |
| Lower Lid Retract, mm |
1 (0 to 1) |
1 (0 to 1) |
1 (0 to 1) |
0.009 |
| Lagopthalmos |
0 (0 to 0) |
0 (0 to 0) |
0 (0 to 1) |
0.058 |
| Lateral Flare |
0 |
0 |
0 |
- |
|
Initial vs 3 rd month |
|
|
|
|
| 1st Fixation |
- |
- |
- |
|
| Palpebral Aperture |
0.196 |
0.316 |
0.413 |
|
| Upper Lid Retract |
0.089 |
0.148 |
0.337 |
|
| Lower Lid Retract |
0.167 |
0.663 |
0.110 |
|
| Lagopthalmos |
0.081 |
0.080 |
- |
|
| Lateral Flare |
- |
- |
- |
|
|
Initial vs 6 th month |
|
|
|
|
| 1st Fixation |
- |
- |
- |
|
| Palpebral Aperture |
0.061 |
0.213 |
0.269 |
|
| Upper Lid Retract |
0.090 |
0.085 |
0.467 |
|
| Lower Lid Retract |
0.002 |
0.008 |
0.114 |
|
| Lagopthalmos |
- |
- |
- |
|
| Lateral Flare |
- |
- |
- |
|
The CAS results are presented in Table 4 and at initial evaluation, spontaneous pain was reported by 15.48% of the total participants, with a significantly higher occurrence in the standard of care group (26.19% vs 4.76%, p = 0.007). Eyelid erythema was present in 4.76% of the total population, with all cases occurring in the standard of care group (9.52% vs 0, p = 0.040). Conjunctival redness on one hand was observed only in the selenium group (9.52% vs 0, p = 0.040). Lastly, caruncle/plical swelling was predominantly observed in the selenium group (33.33% vs 14.29%, p = 0.040). At three-month follow-up, a marked decrease in spontaneous pain was observed in the selenium group, with no participants reporting this symptom, while 26.19% of those in the standard of care group continued to experience it (p<0.001). The CAS scores reflected a significant shift overall, with more eyes having a score of 0 compared to a score of 1 or 2 (p = 0.049). Notably eyelid swelling remained prevalent, but no significant differences were found between the two groups. At the six-month assessment, spontaneous pain continued to be significantly lower in the selenium group (4.76% vs 19.05%, p = 0.043). Eyelid erythema remained significant, as it was noted in 4.76% of the eyes of the total population, all of whom were in the standard of care group (p = 0.040). The CAS scores showed improvement with 47.64% of all participants having a score of zero (p = 0.017), which was highest in frequency in the selenium group at 61.9%. Comparing the initial assessment to three-month evaluation, frequency of caruncle/plical swelling was less overall (23.18% to 8.33%, p = 0.006) and in the selenium group (33.33% to 4.76%, p = 0.005). The CAS scores at this interval also indicated significant improvement in both groups with a score of zero more frequent overall (29.76% to 51.19%, p = 0.016) and in the selenium group (33.33% to 64.29%, p = 0.018). When comparing initial to six-month values, the trend remains consistent, with notable decrease in caruncle/plical swelling and increase in frequency of CAS score of zero overall and in the selenium group.
Table 4. CAS Score
|
Treatment group |
P-value |
|||
|
Total (n=84) |
Selenium (n=42) |
No selenium (control) (n=42) |
||
|
Frequency (%) |
||||
|
Initial |
|
|
|
|
| Spontaneous pain |
13 (15.48) |
2 (4.76) |
11 (26.19) |
0.007 |
| Gaze pain |
2 (2.38) |
0 |
2 (4.76) |
0.152 |
| Eyelid Swelling |
30 (35.71) |
13 (30.95) |
17 (40.48) |
0.62 |
| Eyelid Erythema |
4 (4.76) |
0 |
4 (9.52) |
0.040 |
| Conjunctival Redness |
4 (4.76) |
4 (9.52) |
0 |
0.040 |
| Chemosis |
2 (2.38) |
2 (4.76) |
0 |
0.152 |
| Caruncle/Plical Swelling |
20 (23.81) |
14 (33.33) |
6 (14.29) |
0.040 |
|
CAS score 0 1 2 |
25 (29.76) 43 (51.19) 16 (19.05) |
14 (33.33) 21 (50) 7 (16.67) |
11 (26.19) 22 (52.38) 9 (21.43) |
0.729 |
|
3 rd month |
|
|
|
|
| Spontaneous pain |
11 (13.1) |
0 |
11 (26.19) |
<0.001 |
| Gaze pain |
0 |
0 |
0 |
- |
| Eyelid Swelling |
27 (32.14) |
11 (26.19) |
16 (38.1) |
0.243 |
| Eyelid Erythema |
2 (2.38) |
0 |
2 (4.76) |
0.152 |
| Conjunctival Redness |
4 (4.76) |
2 (4.76) |
2 (4.76) |
1.000 |
| Chemosis |
0 |
0 |
0 |
- |
| Caruncle/Plical Swelling |
7 (8.33) |
3 (7.14) |
4 (9.52) |
0.693 |
| Decreased VA |
3 (3.57) |
3 (7.14) |
0 |
0.078 |
| Increased proptosis |
0 |
0 |
0 |
- |
| Decreased EOMs |
0 |
0 |
0 |
- |
|
CAS score 0 1 2 |
43 (51.19) 28 (33.33) 13 (15.48) |
27 (64.29) 11 (26.19) 4 (9.52) |
16 (38.1) 17 (40.48) 9 (21.43) |
0.049 |
|
6 th month |
|
|
|
|
| Spontaneous pain |
10 (11.9) |
2 (4.76) |
8 (19.05) |
0.043 |
| Gaze pain |
2 (2.38) |
0 |
2 (4.76) |
0.152 |
| Eyelid Swelling |
32 (38.1) |
12 (28.57) |
20 (47.62) |
0.072 |
| Eyelid Erythema |
4 (4.76) |
0 |
4 (9.52) |
0.040 |
| Conjunctival Redness |
2 (2.38) |
0 |
2 (4.76) |
0.152 |
| Chemosis |
0 |
0 |
0 |
- |
| Caruncle/Plical Swelling |
8 (9.52) |
6 (14.29) |
2 (4.76) |
0.137 |
| Decreased VA |
2 (2.38) |
0 |
2 (4.76) |
0.152 |
| Increased proptosis |
0 |
0 |
0 |
- |
| Decreased EOMs |
0 |
0 |
0 |
- |
|
CAS score 0 1 2 |
40 (47.62) 28 (33.33) 16 (19.05) |
26 (61.9) 12 (28.57) 4 (9.52) |
14 (33.33) 16 (38.1) 12 (28.57) |
0.017 |
|
Initial vs 3 rd month (p value) |
|
|
|
|
| Spontaneous pain |
0.659 |
0.494 |
1.000 |
|
| Gaze pain |
0.497 |
- |
0.494 |
|
| Eyelid Swelling |
0.625 |
0.629 |
0.823 |
|
| Eyelid Erythema |
0.406 |
- |
0.397 |
|
| Conjunctival Redness |
1.000 |
0.397 |
0.152 |
|
| Chemosis |
0.497 |
0.494 |
- |
|
| Caruncle/Plical Swelling |
0.006 |
0.005 |
0.738 |
|
| CAS score |
0.016 |
0.018 |
0.457 |
|
|
Initial vs 6 th month (p value) |
|
|
|
|
| Spontaneous pain |
0.501 |
1.000 |
0.434 |
|
| Gaze pain |
1.000 |
- |
1.000 |
|
| Eyelid Swelling |
0.749 |
0.811 |
0.182 |
|
| Eyelid Erythema |
1.000 |
- |
1.000 |
|
| Conjunctival Redness |
0.682 |
0.116 |
0.494 |
|
| Chemosis |
0.155 |
0.494 |
- |
|
| Caruncle/Plical Swelling |
0.013 |
0.040 |
0.265 |
|
| CAS score |
0.036 |
0.033 |
0.420 |
|
Table 5. Number of patients with CAS 0
|
|
Initial |
3 months |
6 months |
|
Selenium |
14 (33.33) |
27 (64.29) |
26 (61.9) |
|
Non-selenium |
11 (26.19) |
16 (38.1) |
14 (33.33) |
The significant difference in caruncle/plical swelling was enough to cause significant difference in CAS between the two groups (selenium and non-selenium) in the third month up to the sixth month with a p-value of 0.016 and 0.036, respectively.
It showed that on initial examination for the selenium group, 14 eyes (33.33%) had a CAS score of 0, which increased to 27 eyes (64.29%) in the third month and ended to a total of 26 eyes (61.9%) at the sixth month of treatment. While for the non-selenium group, 11 eyes had a CAS score of zero initially, increased to 16 eyes (and 38.1%), then finally arrived to a total count of 14 eyes (33.33%).
Table 6. Number of patients with CAS 1
|
|
Initial |
3 months |
6 months |
|
Selenium |
21(50) |
11 (26.19) |
12 (28.57) |
|
Nonselenium |
22(52.38) |
17 (40.48) |
16 (38.1) |
Analyzing the proportion of patients who achieved CAS score 1 among the two groups, it has also been shown how 21 (50) eyes in the selenium group showed statistically significant improvement in terms of decrease in number to 11 and 12 eyes, respectively (26%-28%) for the third and sixth month of treatment.
Table 7. Number of patients with CAS 2
|
CAS score |
Initial |
3 months |
6 months |
|
Selenium |
7 (16.67) |
4 (9.42) |
4(9.52) |
|
Non-selenium |
9 (21.43) |
9 (21.43) |
12(28.57) |
Lastly, the same pattern was observed for CAS 2, wherein a statistically significant decrease in the number of eyes obtaining CAS score 2 was shown in the selenium group, from 7 eyes (16.67) to 4 eyes (9.52). This pattern was not seen in the non-selenium group.
Discussion
This study showed that by the three-month follow-up, the selenium group demonstrated significantly higher BVA and color vision values, but this change was not sustained by the six-month assessment. Significant findings also emerged in eyelid position, particularly lower lid retraction, with the selenium group showing notable improvement compared to the initial assessment. In terms of spontaneous pain, at the onset, this was significantly lower in the selenium group and was further decreased by the three-month period and sustained up to the six-month period. The CAS score indicated overall improvement, with a higher frequency of participants scoring zero in the selenium group at six months. The caruncle/plical swelling decreased significantly in both groups over time, with the selenium group showing a substantial reduction.
These findings align with the study of Marcocci, et al., which demonstrated significantly better overall ophthalmic outcome in patients receiving selenium supplementation compared to the standard care group at the six-month evaluation.[10] In both studies, patients receiving selenium supplementation exhibited a lower CAS and visual acuity remained stable across groups throughout the study periods. Marcocci, et al., also observed significantly lower CAS in the selenium group, corroborating improvements in soft tissue signs and lid retraction in our study.[10] However, the study findings from Kahaly, et al., conducted in Germany, concluded that selenium supplementation did not significantly affect the clinical course or serological parameters in selenium-sufficient hyperthyroid patients with Graves’ disease.[12]
In a more recent study of a cohort of 74 patients, they explored the efficacy of selenium supplementation in patients with mild-to-moderate GO over a five-year period. Those receiving selenium showed significant improvement in symptoms such as tearing, grittiness and conjunctival congestion, as well as better clinical activity and quality of life scores at the six-month follow-up compared to placebo. Selenium also led to a higher rate of improvement and lower rate of worsening in early disease progression. However, while both selenium and placebo groups showed long-term improvement in proptosis and quality of life at the five-year mark, the effects of selenium did not significantly influence long-term outcomes. Thus, as with our study findings, selenium appears beneficial in modifying early GO progression, but does not offer sustained long-term benefits.[13]
One limitation of the current study is the absence of baseline selenium level measurements, which could have provided insight into whether participants were selenium-deficient. This factor might have influenced the efficacy of selenium supplementation in this study. Nevertheless, a study conducted by Wang, et al., in China, involving participants without selenium deficiency, found that selenium supplementation led to decreased thyroglobulin and thyroid-stimulating hormone (TSH) levels, improved quality of life and delayed progression of GO.[14] Additionally, a review by Lanzolla, et al., which included studies with both selenium-sufficient and selenium-deficient participants, concluded that selenium supplementation may positively influence the course of GO.[15]
Last, it is important to note that the study sample size was limited, partly due to challenges posed by the COVID-19 pandemic. Future studies should aim to include large sample sizes to further validate these findings and refine the recommendations for selenium supplementation in the management of mild GO.
Conclusion
Selenium supplementation appears to provide significant short-term benefits, particularly in having better BVA, color vision and reducing spontaneous pain in patients compared to standard of care. The selenium group also showed notable improvements in eyelid position, with a reduction in lower lid retraction and caruncle/plical swelling over time. While the differences in visual improvements were not sustained beyond three months, the continued reduction in pain and inflammatory signs, such as pain and eyelid erythema at six months suggests that selenium may offer longer-term anti-inflammatory benefits. Overall, selenium supplementation shows promise as supportive therapy for improving clinical outcomes, particularly in reducing inflammation and enhancing ocular function in the short-term, though more research is needed to assess its long-term efficacy.
Statement of Authorship
All authors claim fulfillment of International Committee of Medical Journal Editors (ICMJE) authorship criteria.
Credit Author Statement
JMF: Conceptualization, Methodology, Software, Validation, Formal analysis, Investigation, Resources, Data Curation, Writing – original draft preparation, Writing – review and editing, Visualization, Project administration, Funding acquisition;
NADS: Conceptualization, Methodology, Software, Validation, Formal analysis, Investigation, Resources, Data Curation, Writing – original draft preparation, Writing – review and editing, Visualization, Project administration;
JDUH: Conceptualization, Methodology, Validation, Writing – original draft preparation, Writing – review and editing, Visualization, Supervision, Project administration, Funding acquisition;
ASP: Conceptualization, Methodology, Validation, Writing – original draft preparation, Writing – review and editing, Visualization, Supervision,
Author Disclosure
The authors declared no conflict of interest.
Funding Source
2023 Philippine College of Endocrinology Research Grant
-
Gontarz-Nowak K, Szychlińska M, Matuszewski W, Stefanowicz-Rutkowska M, Bandurska-Stankiewicz E. Current knowledge on Graves’ orbitopathy. J Clin Med [Internet]. 2020;10(1):16. Available from: http://dx.doi.org/10.3390/jcm10010016
-
Hiromatsu Y, Eguchi H, Tani J, Kasaoka M, Teshima Y. Graves’ ophthalmopathy: epidemiology and natural history. Intern Med [Internet]. 2014;53(5):353–60. Available from: http://dx.doi.org/10.2169/internalmedicine.53.1518
-
Lat AM, Jauculan MC, Sanchez CA, Jimeno C, Sison-Peña CM, Pe-Yan MR, et al. Risk factors associated with the activity and severity of Graves’ ophthalmopathy among patients at the university of the Philippines manila-Philippine General Hospital. J ASEAN Fed Endocr Soc [Internet]. 2017;32(2):151–7. Available from: http://dx.doi.org/10.15605/jafes.032.02.09
-
Bartalena L, Baldeschi L, Boboridis K, Eckstein A, Kahaly GJ, Marcocci C, et al. The 2016 European thyroid association/European group on Graves’ orbitopathy guidelines for the management of Graves’ orbitopathy. Eur Thyroid J [Internet]. 2016;5(1):9–26. Available from: http://dx.doi.org/10.1159/000443828
-
Chaudhry IA. Thyroid associated orbitopathy: Understanding pathophysiology. Saudi J Ophthalmol [Internet]. 2011;25(1):1–2. Available from: http://dx.doi.org/10.1016/j.sjopt.2010.11.001
-
Bartalena L, Piantanida E, Gallo D, Lai A, Tanda ML. Epidemiology, natural history, risk factors, and prevention of Graves’ orbitopathy. Front Endocrinol (Lausanne) [Internet]. 2020;11:615993. Available from: http://dx.doi.org/10.3389/fendo.2020.615993
-
Palisoc E, Morabe E, Pagkatipunan PM. Prevalence of Graves’ ophthalmopathy among patients with thyroid disease. Philipp J Ophthalmol. 2010;35(1):32–5.
-
Drui D, Du Pasquier Fediaevski L, Vignal Clermont C, Daumerie C. Graves’ orbitopathy: Diagnosis and treatment. Ann Endocrinol (Paris) [Internet]. 2018;79(6):656–64. Available from: http://dx.doi.org/10.1016/j.ando.2018.08.005
-
Bednarczuk T, Schomburg L. Challenges and perspectives of selenium supplementation in Graves’ disease and orbitopathy. Hormones (Athens) [Internet]. 2020;19(1):31–9. Available from: http://dx.doi.org/10.1007/s42000-019-00133-5
-
Bednarczuk T, Schomburg L. Challenges and perspectives of selenium supplementation in Graves’ disease and orbitopathy. Hormones (Athens). 2020;19(1):31–9.
-
Marcocci C, Kahaly GJ, Krassas GE, Bartalena L, Prummel M, Stahl M, et al. Selenium and the course of mild Graves’ orbitopathy. N Engl J Med [Internet]. 2011;364(20):1920–31. Available from: http://dx.doi.org/10.1056/NEJMoa1012985
-
Duffield-Lillico AJ, Slate EH, Reid ME, Turnbull BW, Wilkins PA, Combs GF Jr, et al. Selenium supplementation and secondary prevention of nonmelanoma skin cancer in a randomized trial. J Natl Cancer Inst [Internet]. 2003;95(19):1477–81. Available from: http://dx.doi.org/10.1093/jnci/djg061
-
Kahaly GJ, Riedl M, König J, Diana T, Schomburg L. Double-blind, placebo-controlled, randomized trial of selenium in Graves’ hyperthyroidism. J Clin Endocrinol Metab. 2017;102(11):4333–41.
-
Wang C, Qiao J, Liu S, Piao S, Zhou Y, Hu Y, et al. Selenium in the treatment of mild-to-moderate Graves’ orbitopathy: a 5-year prospective controlled cohort study. Endocrine [Internet]. 2024;84(3):1072–80. Available from: http://dx.doi.org/10.1007/s12020-023-03672-5
-
Wang Y, Patel A, Douglas RS. Thyroid eye disease: How a novel therapy may change the treatment paradigm. Ther Clin Risk Manag [Internet]. 2019;15:1305–18. Available from: http://dx.doi.org/10.2147/TCRM.S193018
-
Lanzolla G, Marinò M, Marcocci C. Selenium in the treatment of Graves’ hyperthyroidism and eye disease. Front Endocrinol (Lausanne) [Internet]. 2020;11:608428. Available from: http://dx.doi.org/10.3389/fendo.2020.608428
APPENDIX 1. EUGOGO GO Quality Of Life Questionnaire

APPENDIX 2: EUGOGO INITIAL ASSESSMENT FORM







APPENDIX 3: EUGOGO Follow up assessment form 





APPENDIX 4: EUGOGO recommendations for assessing response to intervention in clinical trials [18]

APPENDIX 5: EUGOGO severity classification [19]

APPENDIX 6: NO SPECS classification [19]

APPENDIX 7: Clinical Activity Score [20]

![]() Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0
International License, which permits use, share — copy and redistribute the material in any medium or format,
adapt — remix, transform, and build upon the material, as long as you give appropriate credit,
provide a link to the license, and indicate if changes were made. You may do so in any reasonable manner,
but not in any way that suggests the licensor endorses you or your use. You may not use the material for
commercial purposes. If you remix, transform, or build upon the material, you must distribute your
contributions under the same license as the original. You may not apply legal terms or technological
measures that legally restrict others from doing anything the license permits. The images or other
third party material in this article are included in the article’s Creative Commons license, unless indicated
otherwise in a credit line to the material. If material is not included in the article’s Creative Commons
license and your intended use is not permitted by statutory regulation or exceeds the permitted use,
you will need to obtain permission directly from the copyright holder. To view a copy of this license,
visit https://creativecommons.org/licenses/by-nc-sa/4.0/.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0
International License, which permits use, share — copy and redistribute the material in any medium or format,
adapt — remix, transform, and build upon the material, as long as you give appropriate credit,
provide a link to the license, and indicate if changes were made. You may do so in any reasonable manner,
but not in any way that suggests the licensor endorses you or your use. You may not use the material for
commercial purposes. If you remix, transform, or build upon the material, you must distribute your
contributions under the same license as the original. You may not apply legal terms or technological
measures that legally restrict others from doing anything the license permits. The images or other
third party material in this article are included in the article’s Creative Commons license, unless indicated
otherwise in a credit line to the material. If material is not included in the article’s Creative Commons
license and your intended use is not permitted by statutory regulation or exceeds the permitted use,
you will need to obtain permission directly from the copyright holder. To view a copy of this license,
visit https://creativecommons.org/licenses/by-nc-sa/4.0/.